Therese A Stukel, Richard H Glazier, Susan E Schultz, Jun Guan, Brandon M Zagorski, Peter Gozdyra, David A Henry
{"title":"安大略省的多专科医生网络。","authors":"Therese A Stukel, Richard H Glazier, Susan E Schultz, Jun Guan, Brandon M Zagorski, Peter Gozdyra, David A Henry","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Large multispecialty physician group practices, with a central role for primary care practitioners, have been shown to achieve high-quality, low-cost care for patients with chronic disease. We assessed the extent to which informal multispecialty physician networks in Ontario could be identified by using health administrative data to exploit natural linkages among patients, physicians, and hospitals based on existing patient flow.</p><p><strong>Methods: </strong>We linked each Ontario resident to his or her usual provider of primary care over the period from fiscal year 2008/2009 to fiscal year 2010/2011. We linked each specialist to the hospital where he or she performed the most inpatient services. We linked each primary care physician to the hospital where most of his or her ambulatory patients were admitted for non-maternal medical care. Each resident was then linked to the same hospital as his or her usual provider of primary care. We computed \"loyalty\" as the proportion of care to network residents provided by physicians and hospitals within their network. Smaller clusters were aggregated to create networks based on a minimum population size, distance, and loyalty. Networks were not constrained geographically.</p><p><strong>Results: </strong>We identified 78 multispecialty physician networks, comprising 12,410 primary care physicians, 14,687 specialists, and 175 acute care hospitals serving a total of 12,917,178 people. Median network size was 134,723 residents, 125 primary care physicians, and 143 specialists. Virtually all eligible residents were linked to a usual provider of primary care and to a network. Most specialists (93.5%) and primary care physicians (98.2%) were linked to a hospital. Median network physician loyalty was 68.4% for all physician visits and 81.1% for primary care visits. Median non-maternal admission loyalty was 67.4%. Urban networks had lower loyalties and were less self-contained but had more health care resources.</p><p><strong>Interpretation: </strong>We demonstrated the feasibility of identifying informal multispecialty physician networks in Ontario on the basis of patterns of health care-seeking behaviour. Networks were reasonably self-contained, in that individual residents received most of their care from providers within their respective networks. Formal constitution of networks could foster accountability for efficient, integrated care through care management tools and quality improvement, the ideas behind \"accountable care organizations.\"</p>","PeriodicalId":88624,"journal":{"name":"Open medicine : a peer-reviewed, independent, open-access journal","volume":"7 2","pages":"e40-55"},"PeriodicalIF":0.0000,"publicationDate":"2013-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1f/7b/OpenMed-07-e40.PMC3863751.pdf","citationCount":"0","resultStr":"{\"title\":\"Multispecialty physician networks in Ontario.\",\"authors\":\"Therese A Stukel, Richard H Glazier, Susan E Schultz, Jun Guan, Brandon M Zagorski, Peter Gozdyra, David A Henry\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Large multispecialty physician group practices, with a central role for primary care practitioners, have been shown to achieve high-quality, low-cost care for patients with chronic disease. We assessed the extent to which informal multispecialty physician networks in Ontario could be identified by using health administrative data to exploit natural linkages among patients, physicians, and hospitals based on existing patient flow.</p><p><strong>Methods: </strong>We linked each Ontario resident to his or her usual provider of primary care over the period from fiscal year 2008/2009 to fiscal year 2010/2011. We linked each specialist to the hospital where he or she performed the most inpatient services. We linked each primary care physician to the hospital where most of his or her ambulatory patients were admitted for non-maternal medical care. Each resident was then linked to the same hospital as his or her usual provider of primary care. We computed \\\"loyalty\\\" as the proportion of care to network residents provided by physicians and hospitals within their network. Smaller clusters were aggregated to create networks based on a minimum population size, distance, and loyalty. Networks were not constrained geographically.</p><p><strong>Results: </strong>We identified 78 multispecialty physician networks, comprising 12,410 primary care physicians, 14,687 specialists, and 175 acute care hospitals serving a total of 12,917,178 people. Median network size was 134,723 residents, 125 primary care physicians, and 143 specialists. Virtually all eligible residents were linked to a usual provider of primary care and to a network. Most specialists (93.5%) and primary care physicians (98.2%) were linked to a hospital. Median network physician loyalty was 68.4% for all physician visits and 81.1% for primary care visits. Median non-maternal admission loyalty was 67.4%. Urban networks had lower loyalties and were less self-contained but had more health care resources.</p><p><strong>Interpretation: </strong>We demonstrated the feasibility of identifying informal multispecialty physician networks in Ontario on the basis of patterns of health care-seeking behaviour. Networks were reasonably self-contained, in that individual residents received most of their care from providers within their respective networks. Formal constitution of networks could foster accountability for efficient, integrated care through care management tools and quality improvement, the ideas behind \\\"accountable care organizations.\\\"</p>\",\"PeriodicalId\":88624,\"journal\":{\"name\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"volume\":\"7 2\",\"pages\":\"e40-55\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-05-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1f/7b/OpenMed-07-e40.PMC3863751.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2013/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open medicine : a peer-reviewed, independent, open-access journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Background: Large multispecialty physician group practices, with a central role for primary care practitioners, have been shown to achieve high-quality, low-cost care for patients with chronic disease. We assessed the extent to which informal multispecialty physician networks in Ontario could be identified by using health administrative data to exploit natural linkages among patients, physicians, and hospitals based on existing patient flow.
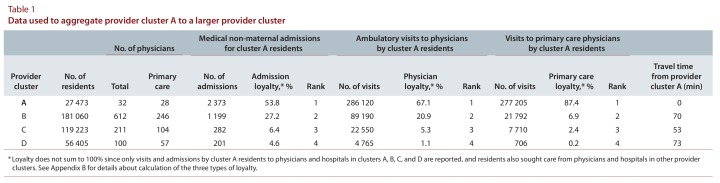
Methods: We linked each Ontario resident to his or her usual provider of primary care over the period from fiscal year 2008/2009 to fiscal year 2010/2011. We linked each specialist to the hospital where he or she performed the most inpatient services. We linked each primary care physician to the hospital where most of his or her ambulatory patients were admitted for non-maternal medical care. Each resident was then linked to the same hospital as his or her usual provider of primary care. We computed "loyalty" as the proportion of care to network residents provided by physicians and hospitals within their network. Smaller clusters were aggregated to create networks based on a minimum population size, distance, and loyalty. Networks were not constrained geographically.
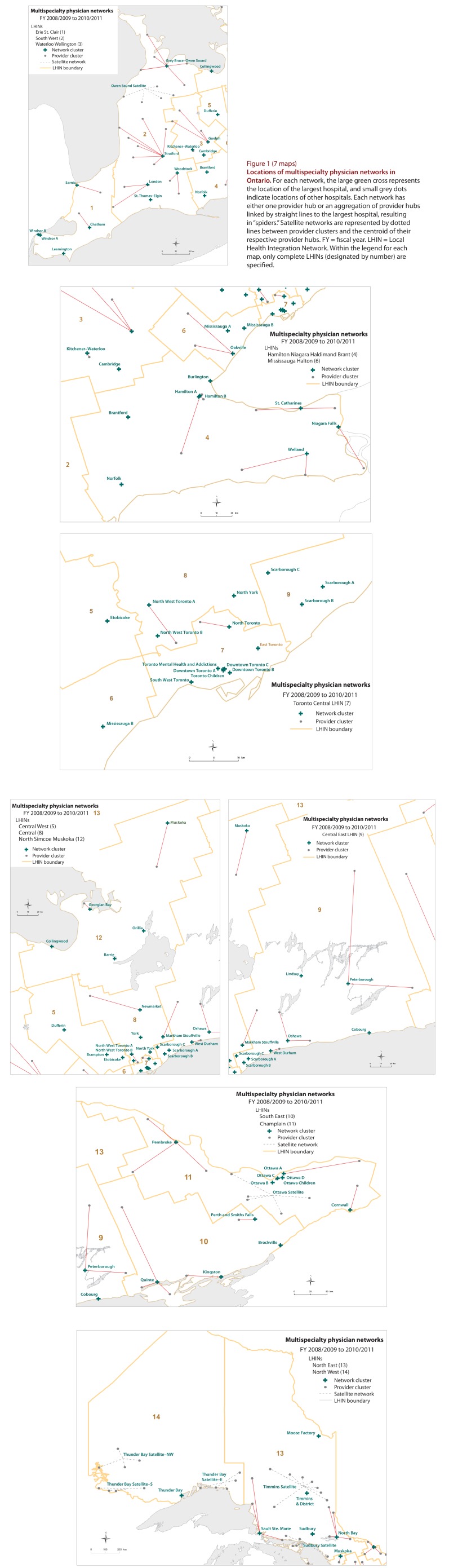
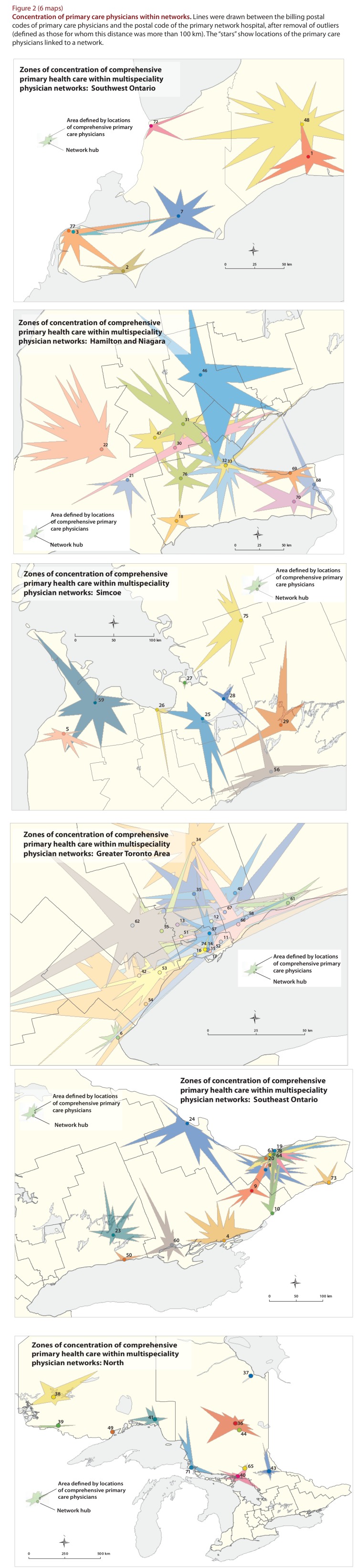
Results: We identified 78 multispecialty physician networks, comprising 12,410 primary care physicians, 14,687 specialists, and 175 acute care hospitals serving a total of 12,917,178 people. Median network size was 134,723 residents, 125 primary care physicians, and 143 specialists. Virtually all eligible residents were linked to a usual provider of primary care and to a network. Most specialists (93.5%) and primary care physicians (98.2%) were linked to a hospital. Median network physician loyalty was 68.4% for all physician visits and 81.1% for primary care visits. Median non-maternal admission loyalty was 67.4%. Urban networks had lower loyalties and were less self-contained but had more health care resources.
Interpretation: We demonstrated the feasibility of identifying informal multispecialty physician networks in Ontario on the basis of patterns of health care-seeking behaviour. Networks were reasonably self-contained, in that individual residents received most of their care from providers within their respective networks. Formal constitution of networks could foster accountability for efficient, integrated care through care management tools and quality improvement, the ideas behind "accountable care organizations."

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


