Hean Teik Ong, Loke Meng Ong, Jacqueline Judith Ho
{"title":"血管紧张素转换酶抑制剂(ACEIs)和血管紧张素受体阻滞剂(ARBs)在高危心血管事件患者中的应用:10项随机安慰剂对照试验的荟萃分析","authors":"Hean Teik Ong, Loke Meng Ong, Jacqueline Judith Ho","doi":"10.1155/2013/478597","DOIUrl":null,"url":null,"abstract":"<p><p>Context. Whether angiotensin converting-enzyme inhibitors (ACEI) and angiotensin-receptor blockers (ARB) are useful in high risk patients without heart failure is unclear. We perform a meta-analysis of prospective randomized placebo-controlled ACEI or ARB trials studying patients with a combination of risk factors to assess treatment impact on all cause mortality, cardiovascular mortality, nonfatal myocardial infarction (MI) and stroke. Method. A PubMed search was made for placebo-controlled trials recruiting at least 1,200 high risk patients randomized to either ACEI or ARB, with follow-up of at least 2 years. Meta-analysis was performed using the RevMan 5 program and Mantel-Haenszel analysis was done with a fixed effects model. Results. Ten trials recruiting 77,633 patients were reviewed. All cause mortality was significantly reduced by ACEI (RR 0.89; P = 0.0008), but not by ARB treatment (RR 1.00; P = 0.89). Cardiovascular mortality and nonfatal MI were also reduced in the ACEI trials but not with ARB therapy. Stroke was significantly reduced in the ACEI trials (RR 0.75; P < 0.00001) and more modestly reduced in the ARB trials (RR 0.90; P = 0.01). Conclusion. ACEI treatment reduced stroke, nonfatal MI, cardiovascular and total mortality in high risk patients, while ARB modestly reduced stroke with no effect on nonfatal MI, cardiovascular and total mortality. </p>","PeriodicalId":73519,"journal":{"name":"ISRN cardiology","volume":"2013 ","pages":"478597"},"PeriodicalIF":0.0000,"publicationDate":"2013-11-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2013/478597","citationCount":"28","resultStr":"{\"title\":\"Angiotensin-Converting Enzyme Inhibitors (ACEIs) and Angiotensin-Receptor Blockers (ARBs) in Patients at High Risk of Cardiovascular Events: A Meta-Analysis of 10 Randomised Placebo-Controlled Trials.\",\"authors\":\"Hean Teik Ong, Loke Meng Ong, Jacqueline Judith Ho\",\"doi\":\"10.1155/2013/478597\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Context. Whether angiotensin converting-enzyme inhibitors (ACEI) and angiotensin-receptor blockers (ARB) are useful in high risk patients without heart failure is unclear. We perform a meta-analysis of prospective randomized placebo-controlled ACEI or ARB trials studying patients with a combination of risk factors to assess treatment impact on all cause mortality, cardiovascular mortality, nonfatal myocardial infarction (MI) and stroke. Method. A PubMed search was made for placebo-controlled trials recruiting at least 1,200 high risk patients randomized to either ACEI or ARB, with follow-up of at least 2 years. Meta-analysis was performed using the RevMan 5 program and Mantel-Haenszel analysis was done with a fixed effects model. Results. Ten trials recruiting 77,633 patients were reviewed. All cause mortality was significantly reduced by ACEI (RR 0.89; P = 0.0008), but not by ARB treatment (RR 1.00; P = 0.89). Cardiovascular mortality and nonfatal MI were also reduced in the ACEI trials but not with ARB therapy. Stroke was significantly reduced in the ACEI trials (RR 0.75; P < 0.00001) and more modestly reduced in the ARB trials (RR 0.90; P = 0.01). Conclusion. ACEI treatment reduced stroke, nonfatal MI, cardiovascular and total mortality in high risk patients, while ARB modestly reduced stroke with no effect on nonfatal MI, cardiovascular and total mortality. </p>\",\"PeriodicalId\":73519,\"journal\":{\"name\":\"ISRN cardiology\",\"volume\":\"2013 \",\"pages\":\"478597\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-11-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2013/478597\",\"citationCount\":\"28\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ISRN cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2013/478597\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ISRN cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2013/478597","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Angiotensin-Converting Enzyme Inhibitors (ACEIs) and Angiotensin-Receptor Blockers (ARBs) in Patients at High Risk of Cardiovascular Events: A Meta-Analysis of 10 Randomised Placebo-Controlled Trials.
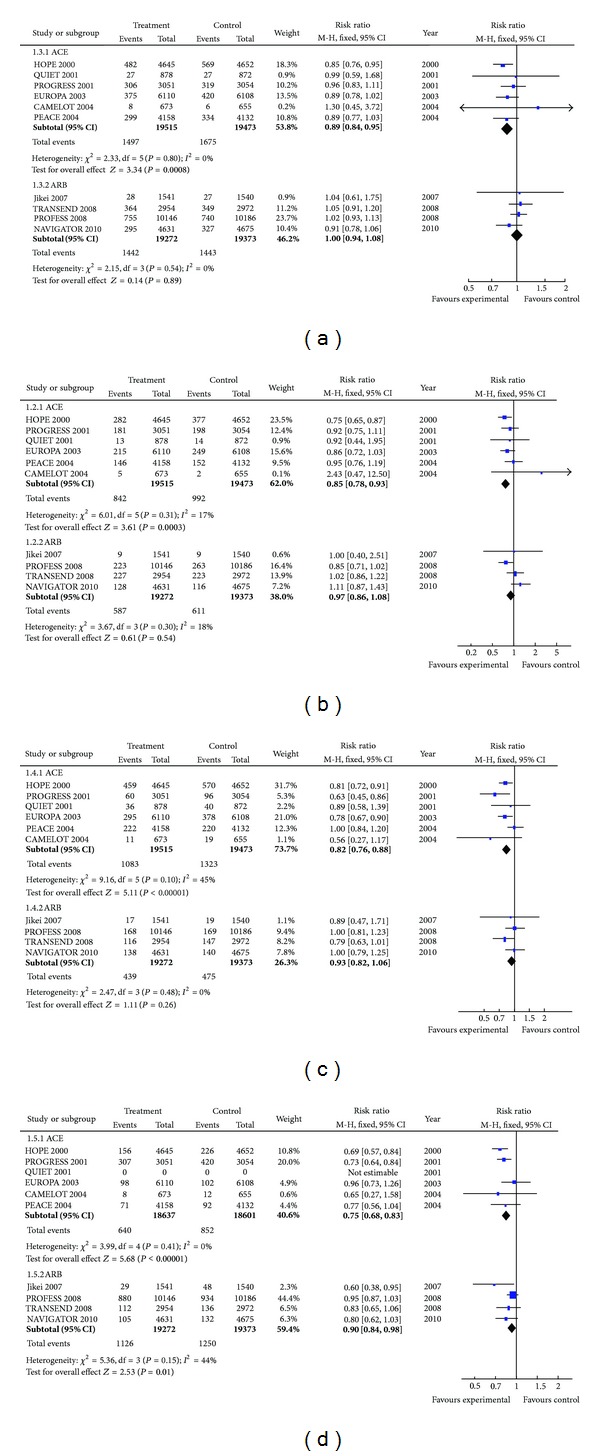
Context. Whether angiotensin converting-enzyme inhibitors (ACEI) and angiotensin-receptor blockers (ARB) are useful in high risk patients without heart failure is unclear. We perform a meta-analysis of prospective randomized placebo-controlled ACEI or ARB trials studying patients with a combination of risk factors to assess treatment impact on all cause mortality, cardiovascular mortality, nonfatal myocardial infarction (MI) and stroke. Method. A PubMed search was made for placebo-controlled trials recruiting at least 1,200 high risk patients randomized to either ACEI or ARB, with follow-up of at least 2 years. Meta-analysis was performed using the RevMan 5 program and Mantel-Haenszel analysis was done with a fixed effects model. Results. Ten trials recruiting 77,633 patients were reviewed. All cause mortality was significantly reduced by ACEI (RR 0.89; P = 0.0008), but not by ARB treatment (RR 1.00; P = 0.89). Cardiovascular mortality and nonfatal MI were also reduced in the ACEI trials but not with ARB therapy. Stroke was significantly reduced in the ACEI trials (RR 0.75; P < 0.00001) and more modestly reduced in the ARB trials (RR 0.90; P = 0.01). Conclusion. ACEI treatment reduced stroke, nonfatal MI, cardiovascular and total mortality in high risk patients, while ARB modestly reduced stroke with no effect on nonfatal MI, cardiovascular and total mortality.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


