Thomas P Olson, Dustin L Denzer, William L Sinnett, Ted Wilson, Bruce D Johnson
{"title":"静息肺功能对心力衰竭的预后价值。","authors":"Thomas P Olson, Dustin L Denzer, William L Sinnett, Ted Wilson, Bruce D Johnson","doi":"10.4137/CCRPM.S12525","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The heart and lungs are intimately linked anatomically and physiologically, and, as a result, heart failure (HF) patients often develop changes in pulmonary function. This study examined the prognostic value of resting pulmonary function (PF) in HF.</p><p><strong>Methods and results: </strong>In all, 134 HF patients (enrolled from January 1, 1999 Through December 31, 2005; ejection fraction (EF) = 29% ± 11%; mean age = 55 ± 12 years; 65% male) were followed for 67 ± 34 months with death/transplant confirmed via the Social Security Index and Mayo Clinic registry. PF included forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), diffusing capacity of the lungs for carbon monoxide (DLCO), and alveolar volume (VA). Patients were divided in tertiles according to PF with survival analysis via log-rank Mantel-Cox test with chi-square analysis. Groups for FVC included (1) >96%, (2) 96% to 81%, and (3) <81% predicted (chi-square = 18.9, P < 0.001). Bonferroni correction for multiple comparisons (BC) suggested differences between groups 1 and 3 (P < 0.001) and 2 and 3 (P = 0.008). Groups for FEV1 included (1) >94%, (2) 94% to 77%, and (3) <77% predicted (chi-square = 17.3, P <0.001). BC suggested differences between groups 1 and 3 (P <0.001). Groups for DLCO included (1) >90%, (2) 90% to 75%, and (3) <75% predicted (chi-square = 11.9, P = 0.003). BC suggested differences between groups 1 and 3 (P < 0.001). Groups for VA included (1) >97%, (2) 97% to 87%, and (3) <87% predicted (Chi-square = 8.5, P = 0.01). BC suggested differences between groups 1 and 2 (P = 0.014) and 1 and 3 (P = 0.003).</p><p><strong>Conclusions: </strong>In a well-defined cohort of HF patients, resting measures of PF are predictive of all-cause mortality.</p>","PeriodicalId":44269,"journal":{"name":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","volume":"7 ","pages":"35-43"},"PeriodicalIF":1.0000,"publicationDate":"2013-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4137/CCRPM.S12525","citationCount":"22","resultStr":"{\"title\":\"Prognostic value of resting pulmonary function in heart failure.\",\"authors\":\"Thomas P Olson, Dustin L Denzer, William L Sinnett, Ted Wilson, Bruce D Johnson\",\"doi\":\"10.4137/CCRPM.S12525\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The heart and lungs are intimately linked anatomically and physiologically, and, as a result, heart failure (HF) patients often develop changes in pulmonary function. This study examined the prognostic value of resting pulmonary function (PF) in HF.</p><p><strong>Methods and results: </strong>In all, 134 HF patients (enrolled from January 1, 1999 Through December 31, 2005; ejection fraction (EF) = 29% ± 11%; mean age = 55 ± 12 years; 65% male) were followed for 67 ± 34 months with death/transplant confirmed via the Social Security Index and Mayo Clinic registry. PF included forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), diffusing capacity of the lungs for carbon monoxide (DLCO), and alveolar volume (VA). Patients were divided in tertiles according to PF with survival analysis via log-rank Mantel-Cox test with chi-square analysis. Groups for FVC included (1) >96%, (2) 96% to 81%, and (3) <81% predicted (chi-square = 18.9, P < 0.001). Bonferroni correction for multiple comparisons (BC) suggested differences between groups 1 and 3 (P < 0.001) and 2 and 3 (P = 0.008). Groups for FEV1 included (1) >94%, (2) 94% to 77%, and (3) <77% predicted (chi-square = 17.3, P <0.001). BC suggested differences between groups 1 and 3 (P <0.001). Groups for DLCO included (1) >90%, (2) 90% to 75%, and (3) <75% predicted (chi-square = 11.9, P = 0.003). BC suggested differences between groups 1 and 3 (P < 0.001). Groups for VA included (1) >97%, (2) 97% to 87%, and (3) <87% predicted (Chi-square = 8.5, P = 0.01). BC suggested differences between groups 1 and 2 (P = 0.014) and 1 and 3 (P = 0.003).</p><p><strong>Conclusions: </strong>In a well-defined cohort of HF patients, resting measures of PF are predictive of all-cause mortality.</p>\",\"PeriodicalId\":44269,\"journal\":{\"name\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"volume\":\"7 \",\"pages\":\"35-43\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2013-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.4137/CCRPM.S12525\",\"citationCount\":\"22\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4137/CCRPM.S12525\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2013/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4137/CCRPM.S12525","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Prognostic value of resting pulmonary function in heart failure.
Background: The heart and lungs are intimately linked anatomically and physiologically, and, as a result, heart failure (HF) patients often develop changes in pulmonary function. This study examined the prognostic value of resting pulmonary function (PF) in HF.
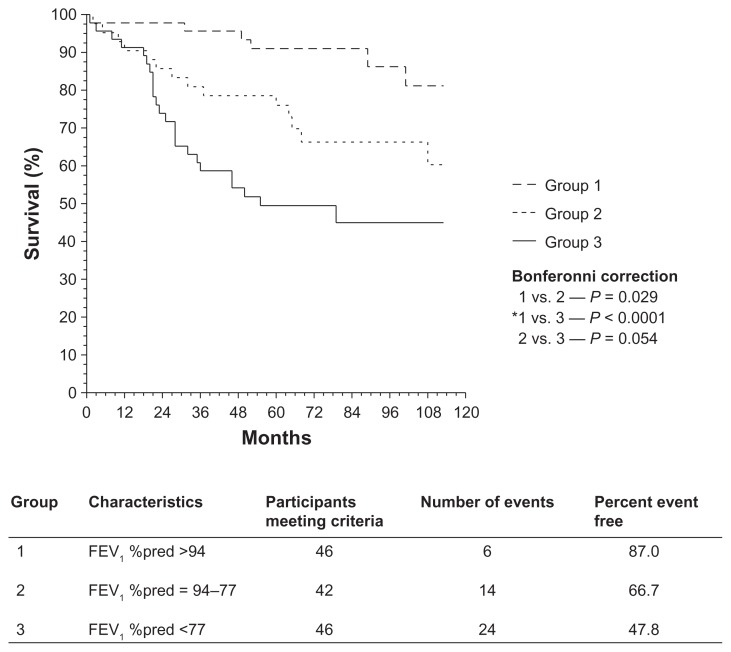
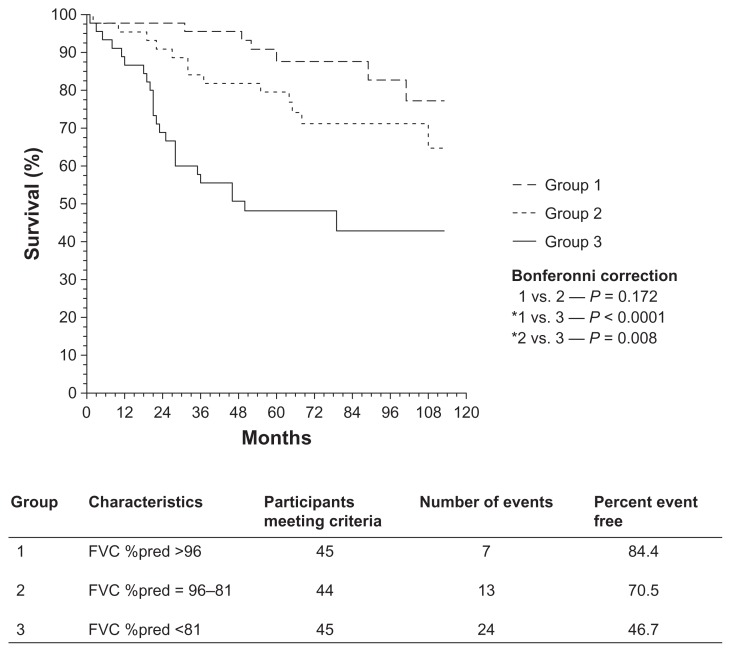
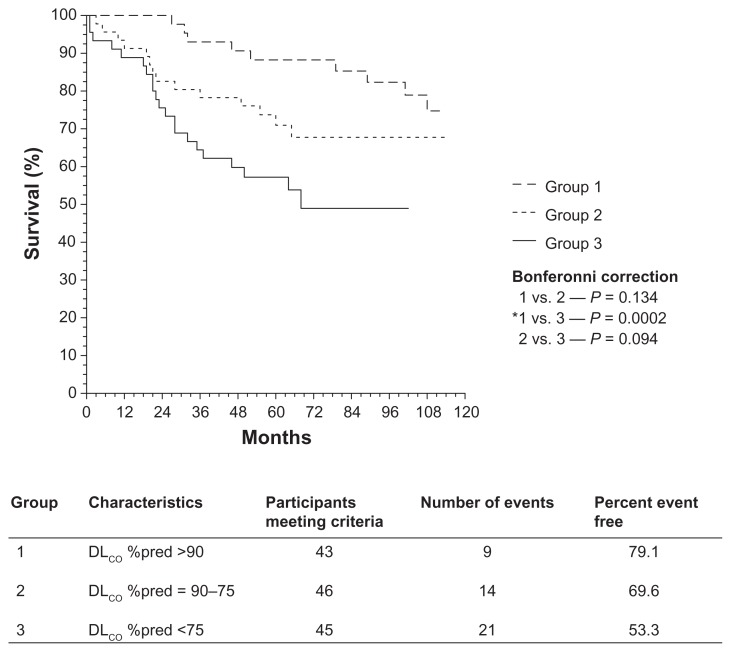
Methods and results: In all, 134 HF patients (enrolled from January 1, 1999 Through December 31, 2005; ejection fraction (EF) = 29% ± 11%; mean age = 55 ± 12 years; 65% male) were followed for 67 ± 34 months with death/transplant confirmed via the Social Security Index and Mayo Clinic registry. PF included forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), diffusing capacity of the lungs for carbon monoxide (DLCO), and alveolar volume (VA). Patients were divided in tertiles according to PF with survival analysis via log-rank Mantel-Cox test with chi-square analysis. Groups for FVC included (1) >96%, (2) 96% to 81%, and (3) <81% predicted (chi-square = 18.9, P < 0.001). Bonferroni correction for multiple comparisons (BC) suggested differences between groups 1 and 3 (P < 0.001) and 2 and 3 (P = 0.008). Groups for FEV1 included (1) >94%, (2) 94% to 77%, and (3) <77% predicted (chi-square = 17.3, P <0.001). BC suggested differences between groups 1 and 3 (P <0.001). Groups for DLCO included (1) >90%, (2) 90% to 75%, and (3) <75% predicted (chi-square = 11.9, P = 0.003). BC suggested differences between groups 1 and 3 (P < 0.001). Groups for VA included (1) >97%, (2) 97% to 87%, and (3) <87% predicted (Chi-square = 8.5, P = 0.01). BC suggested differences between groups 1 and 2 (P = 0.014) and 1 and 3 (P = 0.003).
Conclusions: In a well-defined cohort of HF patients, resting measures of PF are predictive of all-cause mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


