Leah S Steele, Anna Durbin, Lyn M Sibley, Richard Glazier
{"title":"将精神病患者纳入以患者为中心的医疗之家:来自加拿大安大略省的横断面调查结果。","authors":"Leah S Steele, Anna Durbin, Lyn M Sibley, Richard Glazier","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In Ontario, Canada, the patient-centred medical home is a model of primary care delivery that includes 3 model types of interest for this study: enhanced fee-for-service, blended capitation, and team-based blended capitation. All 3 models involve rostering of patients and have similar practice requirements but differ in method of physician reimbursement, with the blended capitation models incorporating adjustments for age and sex, but not case mix, of rostered patients. We evaluated the extent to which persons with mental illness were included in physicians' total practices (as rostered and non-rostered patients) and were included on physicians' rosters across types of medical homes in Ontario.</p><p><strong>Methods: </strong>Using population-based administrative data, we considered 3 groups of patients: those with psychotic or bipolar diagnoses, those with other mental health diagnoses, and those with no mental health diagnoses. We modelled the prevalence of mental health diagnoses and the proportion of patients with such diagnoses who were rostered across the 3 medical home model types, controlling for demographic characteristics and case mix.</p><p><strong>Results: </strong>Compared with enhanced fee-for-service practices, and relative to patients without mental illness, the proportions of patients with psychosis or bipolar disorders were not different in blended capitation and team-based blended capitation practices (rate ratio [RR] 0.91, 95% confidence interval [CI] 0.82-1.01; RR 1.06, 95% CI 0.96-1.17, respectively). However, there were fewer patients with other mental illnesses (RR 0.94, 95% CI 0.90-0.99; RR 0.89, 95% CI 0.85-0.94, respectively). Compared with expected proportions, practices based on both capitation models were significantly less likely than enhanced fee-for-service practices to roster patients with psychosis or bipolar disorders (for blended capitation, RR 0.92, 95% CI 0.90-0.93; for team-based capitation, RR 0.92, 95% CI 0.88-0.93) and also patients with other mental illnesses (for blended capitation, RR 0.94, 95% CI 0.92-0.95; for team-based capitation, RR 0.93, 95% CI 0.92-0.94).</p><p><strong>Interpretation: </strong>Persons with mental illness were under-represented in the rosters of Ontario's capitation-based medical homes. These findings suggest a need to direct attention to the incentive structure for including patients with mental illness.</p>","PeriodicalId":88624,"journal":{"name":"Open medicine : a peer-reviewed, independent, open-access journal","volume":"7 1","pages":"e9-20"},"PeriodicalIF":0.0000,"publicationDate":"2013-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/da/af/OpenMed-07-e9.PMC3654503.pdf","citationCount":"0","resultStr":"{\"title\":\"Inclusion of persons with mental illness in patient-centred medical homes: cross-sectional findings from Ontario, Canada.\",\"authors\":\"Leah S Steele, Anna Durbin, Lyn M Sibley, Richard Glazier\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In Ontario, Canada, the patient-centred medical home is a model of primary care delivery that includes 3 model types of interest for this study: enhanced fee-for-service, blended capitation, and team-based blended capitation. All 3 models involve rostering of patients and have similar practice requirements but differ in method of physician reimbursement, with the blended capitation models incorporating adjustments for age and sex, but not case mix, of rostered patients. We evaluated the extent to which persons with mental illness were included in physicians' total practices (as rostered and non-rostered patients) and were included on physicians' rosters across types of medical homes in Ontario.</p><p><strong>Methods: </strong>Using population-based administrative data, we considered 3 groups of patients: those with psychotic or bipolar diagnoses, those with other mental health diagnoses, and those with no mental health diagnoses. We modelled the prevalence of mental health diagnoses and the proportion of patients with such diagnoses who were rostered across the 3 medical home model types, controlling for demographic characteristics and case mix.</p><p><strong>Results: </strong>Compared with enhanced fee-for-service practices, and relative to patients without mental illness, the proportions of patients with psychosis or bipolar disorders were not different in blended capitation and team-based blended capitation practices (rate ratio [RR] 0.91, 95% confidence interval [CI] 0.82-1.01; RR 1.06, 95% CI 0.96-1.17, respectively). However, there were fewer patients with other mental illnesses (RR 0.94, 95% CI 0.90-0.99; RR 0.89, 95% CI 0.85-0.94, respectively). Compared with expected proportions, practices based on both capitation models were significantly less likely than enhanced fee-for-service practices to roster patients with psychosis or bipolar disorders (for blended capitation, RR 0.92, 95% CI 0.90-0.93; for team-based capitation, RR 0.92, 95% CI 0.88-0.93) and also patients with other mental illnesses (for blended capitation, RR 0.94, 95% CI 0.92-0.95; for team-based capitation, RR 0.93, 95% CI 0.92-0.94).</p><p><strong>Interpretation: </strong>Persons with mental illness were under-represented in the rosters of Ontario's capitation-based medical homes. These findings suggest a need to direct attention to the incentive structure for including patients with mental illness.</p>\",\"PeriodicalId\":88624,\"journal\":{\"name\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"volume\":\"7 1\",\"pages\":\"e9-20\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-02-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/da/af/OpenMed-07-e9.PMC3654503.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2013/1/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open medicine : a peer-reviewed, independent, open-access journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:在加拿大安大略省,以患者为中心的医疗之家是一种初级保健服务模式,包括本研究感兴趣的3种模式类型:强化服务收费、混合收费和基于团队的混合收费。所有三种模式都涉及患者名册,具有相似的实践要求,但在医生报销方法上有所不同,混合人头模型纳入了名册患者的年龄和性别调整,但没有病例混合。我们评估了精神疾病患者被纳入医生总实践的程度(作为名册患者和非名册患者),并被纳入安大略省各类医疗之家的医生名册。方法:使用基于人群的管理数据,我们考虑了3组患者:精神病或双相情感障碍诊断,其他精神健康诊断和无精神健康诊断。我们模拟了心理健康诊断的流行程度以及在3种医疗家庭模型类型中登记的此类诊断的患者比例,控制了人口统计学特征和病例组合。结果:与强化的按服务收费的做法相比,相对于无精神疾病的患者,混合医疗和团队为基础的混合医疗中精神病或双相情感障碍患者的比例没有差异(比率比[RR] 0.91, 95%可信区间[CI] 0.82-1.01;RR 1.06, 95% CI 0.96-1.17)。然而,有其他精神疾病的患者较少(RR 0.94, 95% CI 0.90-0.99;RR 0.89, 95% CI 0.85-0.94)。与预期比例相比,基于两种计费模式的做法比基于服务付费模式的做法更不可能将精神病或双相情感障碍患者列入名册(对于混合计费模式,RR 0.92, 95% CI 0.90-0.93;以团队为基础的起头,RR 0.92, 95% CI 0.88-0.93)以及其他精神疾病患者(混合起头,RR 0.94, 95% CI 0.92-0.95;团队资本化,RR 0.93, 95% CI 0.92-0.94)。解释:安大略省首府医疗之家名册中精神病患者人数不足。这些发现表明,有必要将注意力集中在包括精神疾病患者的激励结构上。
Inclusion of persons with mental illness in patient-centred medical homes: cross-sectional findings from Ontario, Canada.
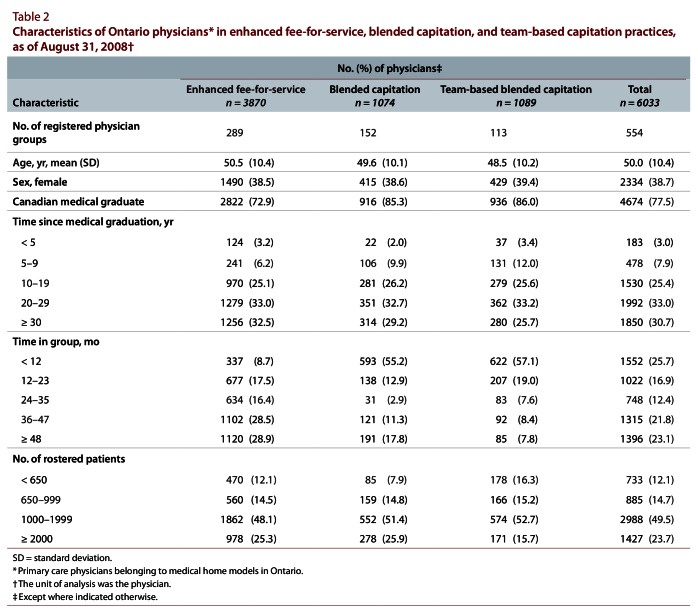
Background: In Ontario, Canada, the patient-centred medical home is a model of primary care delivery that includes 3 model types of interest for this study: enhanced fee-for-service, blended capitation, and team-based blended capitation. All 3 models involve rostering of patients and have similar practice requirements but differ in method of physician reimbursement, with the blended capitation models incorporating adjustments for age and sex, but not case mix, of rostered patients. We evaluated the extent to which persons with mental illness were included in physicians' total practices (as rostered and non-rostered patients) and were included on physicians' rosters across types of medical homes in Ontario.
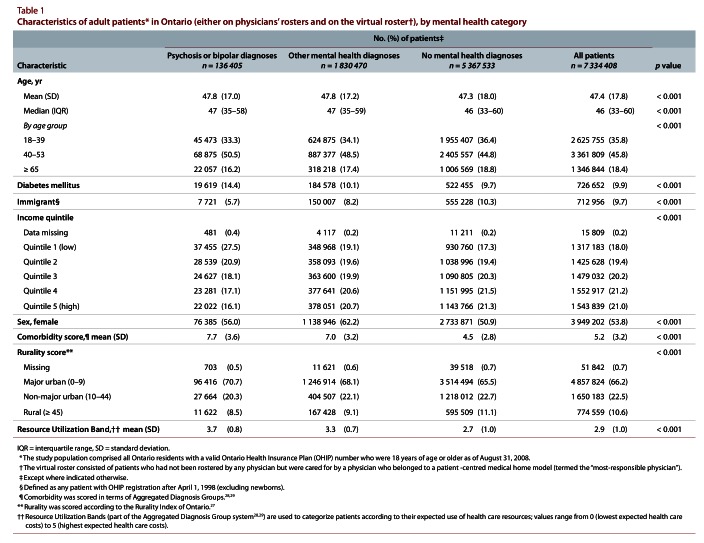
Methods: Using population-based administrative data, we considered 3 groups of patients: those with psychotic or bipolar diagnoses, those with other mental health diagnoses, and those with no mental health diagnoses. We modelled the prevalence of mental health diagnoses and the proportion of patients with such diagnoses who were rostered across the 3 medical home model types, controlling for demographic characteristics and case mix.
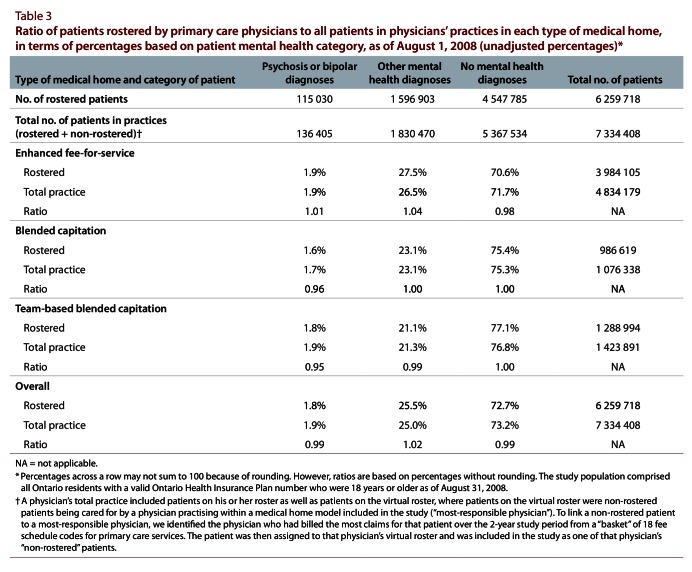
Results: Compared with enhanced fee-for-service practices, and relative to patients without mental illness, the proportions of patients with psychosis or bipolar disorders were not different in blended capitation and team-based blended capitation practices (rate ratio [RR] 0.91, 95% confidence interval [CI] 0.82-1.01; RR 1.06, 95% CI 0.96-1.17, respectively). However, there were fewer patients with other mental illnesses (RR 0.94, 95% CI 0.90-0.99; RR 0.89, 95% CI 0.85-0.94, respectively). Compared with expected proportions, practices based on both capitation models were significantly less likely than enhanced fee-for-service practices to roster patients with psychosis or bipolar disorders (for blended capitation, RR 0.92, 95% CI 0.90-0.93; for team-based capitation, RR 0.92, 95% CI 0.88-0.93) and also patients with other mental illnesses (for blended capitation, RR 0.94, 95% CI 0.92-0.95; for team-based capitation, RR 0.93, 95% CI 0.92-0.94).
Interpretation: Persons with mental illness were under-represented in the rosters of Ontario's capitation-based medical homes. These findings suggest a need to direct attention to the incentive structure for including patients with mental illness.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


