Paul E Ronksley, Claudia Sanmartin, Hude Quan, Pietro Ravani, Marcello Tonelli, Braden Manns, Brenda R Hemmelgarn
{"title":"感知未满足的卫生保健需求与慢性疾病患者不良健康结局风险之间的关系","authors":"Paul E Ronksley, Claudia Sanmartin, Hude Quan, Pietro Ravani, Marcello Tonelli, Braden Manns, Brenda R Hemmelgarn","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adults with chronic medical conditions are more likely to report unmet health care needs. Whether unmet health care needs are associated with an increased risk of adverse health outcomes is unclear.</p><p><strong>Methods: </strong>Adults with at least one self-reported chronic condition (arthritis, chronic obstructive pulmonary disease, diabetes mellitus, heart disease, hypertension, mood disorder, stroke) from the 2001 and 2003 cycles of the Canadian Community Health Survey were linked to national hospitalization data. Participants were followed from the date of their survey until March 31, 2005, for the primary outcomes of all-cause and cause-specific admission to hospital. Secondary outcomes included length of stay, 30-day and 1-year all-cause readmission to hospital, and in-hospital death. Negative binomial regression models were used to estimate the association between unmet health care needs, admission to hospital, and length of stay, with adjustment for socio-demographic variables, health behaviours, and health status. Logistic regression was used to estimate the association between unmet needs, readmission, and in-hospital death. Further analyses were conducted by type of unmet need.</p><p><strong>Results: </strong>Of the 51 932 adults with self-reported chronic disease, 15.5% reported an unmet health care need. Participants with unmet health care needs had a risk of all-cause admission to hospital similar to that of patients with no unmet needs (adjusted rate ratio [RR] 1.04, 95% confidence interval [CI] 0.94-1.15). When stratified by type of need, participants who reported issues of limited resource availability had a slightly higher risk of hospital admission (RR 1.18, 95% CI 1.09-1.28). There was no association between unmet needs and length of stay, readmission, or in-hospital death.</p><p><strong>Interpretation: </strong>Overall, unmet health care needs were not associated with an increased risk of admission to hospital among those with chronic conditions. However, certain types of unmet needs may be associated with higher or lower risk. Whether unmet needs are associated with other measures of resource use remains to be determined.</p>","PeriodicalId":88624,"journal":{"name":"Open medicine : a peer-reviewed, independent, open-access journal","volume":"7 1","pages":"e21-30"},"PeriodicalIF":0.0000,"publicationDate":"2013-02-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/f8/OpenMed-07-e21.PMC3654502.pdf","citationCount":"0","resultStr":"{\"title\":\"Association between perceived unmet health care needs and risk of adverse health outcomes among patients with chronic medical conditions.\",\"authors\":\"Paul E Ronksley, Claudia Sanmartin, Hude Quan, Pietro Ravani, Marcello Tonelli, Braden Manns, Brenda R Hemmelgarn\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Adults with chronic medical conditions are more likely to report unmet health care needs. Whether unmet health care needs are associated with an increased risk of adverse health outcomes is unclear.</p><p><strong>Methods: </strong>Adults with at least one self-reported chronic condition (arthritis, chronic obstructive pulmonary disease, diabetes mellitus, heart disease, hypertension, mood disorder, stroke) from the 2001 and 2003 cycles of the Canadian Community Health Survey were linked to national hospitalization data. Participants were followed from the date of their survey until March 31, 2005, for the primary outcomes of all-cause and cause-specific admission to hospital. Secondary outcomes included length of stay, 30-day and 1-year all-cause readmission to hospital, and in-hospital death. Negative binomial regression models were used to estimate the association between unmet health care needs, admission to hospital, and length of stay, with adjustment for socio-demographic variables, health behaviours, and health status. Logistic regression was used to estimate the association between unmet needs, readmission, and in-hospital death. Further analyses were conducted by type of unmet need.</p><p><strong>Results: </strong>Of the 51 932 adults with self-reported chronic disease, 15.5% reported an unmet health care need. Participants with unmet health care needs had a risk of all-cause admission to hospital similar to that of patients with no unmet needs (adjusted rate ratio [RR] 1.04, 95% confidence interval [CI] 0.94-1.15). When stratified by type of need, participants who reported issues of limited resource availability had a slightly higher risk of hospital admission (RR 1.18, 95% CI 1.09-1.28). There was no association between unmet needs and length of stay, readmission, or in-hospital death.</p><p><strong>Interpretation: </strong>Overall, unmet health care needs were not associated with an increased risk of admission to hospital among those with chronic conditions. However, certain types of unmet needs may be associated with higher or lower risk. Whether unmet needs are associated with other measures of resource use remains to be determined.</p>\",\"PeriodicalId\":88624,\"journal\":{\"name\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"volume\":\"7 1\",\"pages\":\"e21-30\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-02-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/f8/OpenMed-07-e21.PMC3654502.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2013/1/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open medicine : a peer-reviewed, independent, open-access journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:患有慢性疾病的成年人更有可能报告未满足的卫生保健需求。未满足的卫生保健需求是否与不良健康结果风险增加有关尚不清楚。方法:2001年和2003年加拿大社区健康调查周期中自我报告至少有一种慢性疾病(关节炎、慢性阻塞性肺病、糖尿病、心脏病、高血压、情绪障碍、中风)的成年人与全国住院数据相关联。从调查之日起至2005年3月31日,对参与者进行随访,以了解所有原因和特定原因住院的主要结果。次要结局包括住院时间、30天和1年全因再入院以及院内死亡。使用负二项回归模型来估计未满足的医疗保健需求、住院率和住院时间之间的关系,并对社会人口统计学变量、健康行为和健康状况进行调整。采用Logistic回归估计未满足需求、再入院和院内死亡之间的关系。根据未满足需求的类型进行了进一步的分析。结果:在51 932名自我报告患有慢性疾病的成年人中,15.5%的人报告了未满足的卫生保健需求。未满足医疗保健需求的参与者与未满足医疗保健需求的患者的全因住院风险相似(调整比率比[RR] 1.04, 95%可信区间[CI] 0.94-1.15)。当按需求类型分层时,报告资源可用性有限问题的参与者入院的风险略高(RR 1.18, 95% CI 1.09-1.28)。未满足的需求与住院时间、再入院或院内死亡之间没有关联。解释:总体而言,未满足的卫生保健需求与慢性病患者入院风险增加无关。然而,某些类型的未满足需求可能与更高或更低的风险相关。未满足的需求是否与其他资源使用措施有关,仍有待确定。
Association between perceived unmet health care needs and risk of adverse health outcomes among patients with chronic medical conditions.
Background: Adults with chronic medical conditions are more likely to report unmet health care needs. Whether unmet health care needs are associated with an increased risk of adverse health outcomes is unclear.
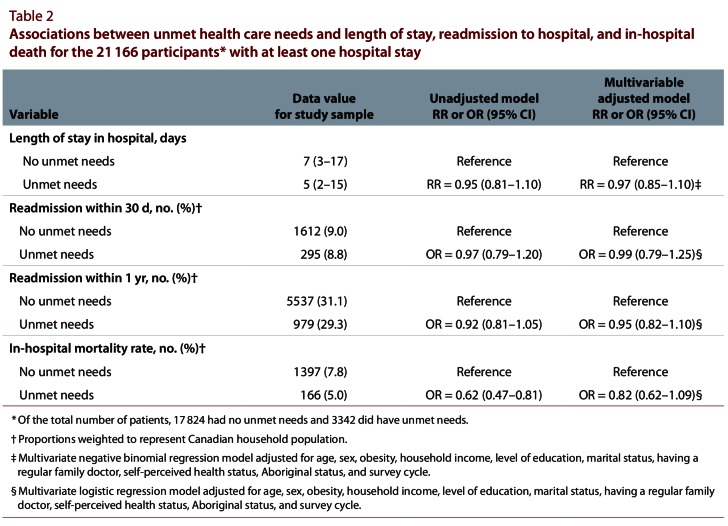
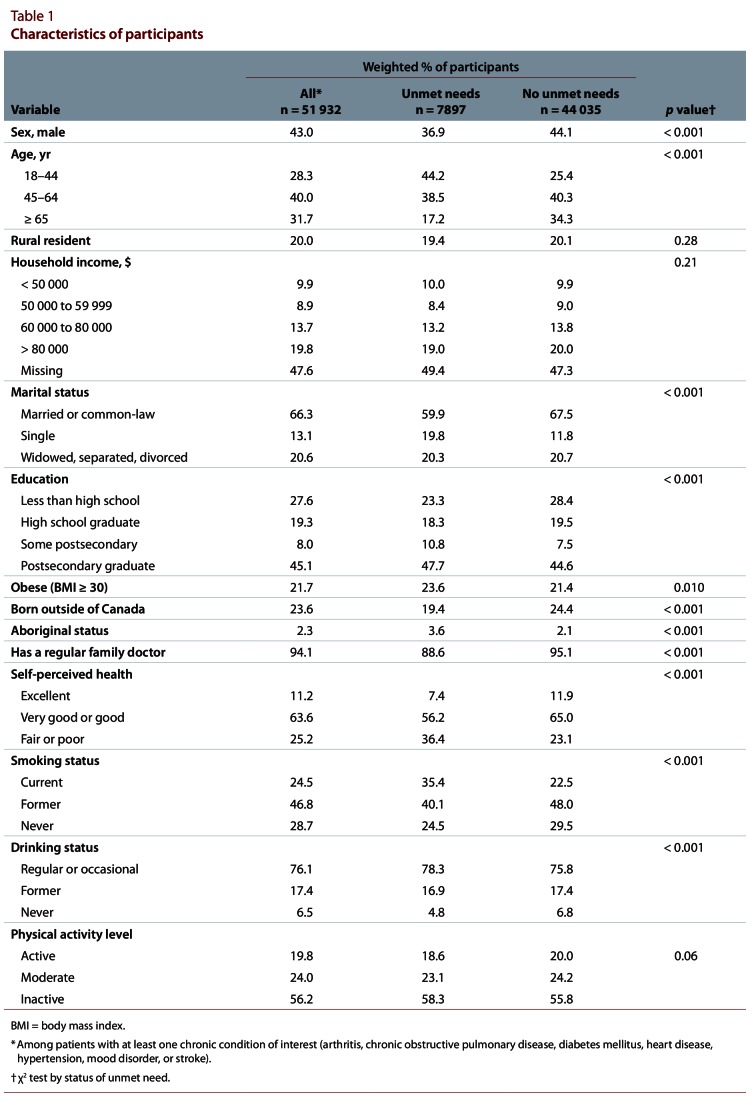
Methods: Adults with at least one self-reported chronic condition (arthritis, chronic obstructive pulmonary disease, diabetes mellitus, heart disease, hypertension, mood disorder, stroke) from the 2001 and 2003 cycles of the Canadian Community Health Survey were linked to national hospitalization data. Participants were followed from the date of their survey until March 31, 2005, for the primary outcomes of all-cause and cause-specific admission to hospital. Secondary outcomes included length of stay, 30-day and 1-year all-cause readmission to hospital, and in-hospital death. Negative binomial regression models were used to estimate the association between unmet health care needs, admission to hospital, and length of stay, with adjustment for socio-demographic variables, health behaviours, and health status. Logistic regression was used to estimate the association between unmet needs, readmission, and in-hospital death. Further analyses were conducted by type of unmet need.
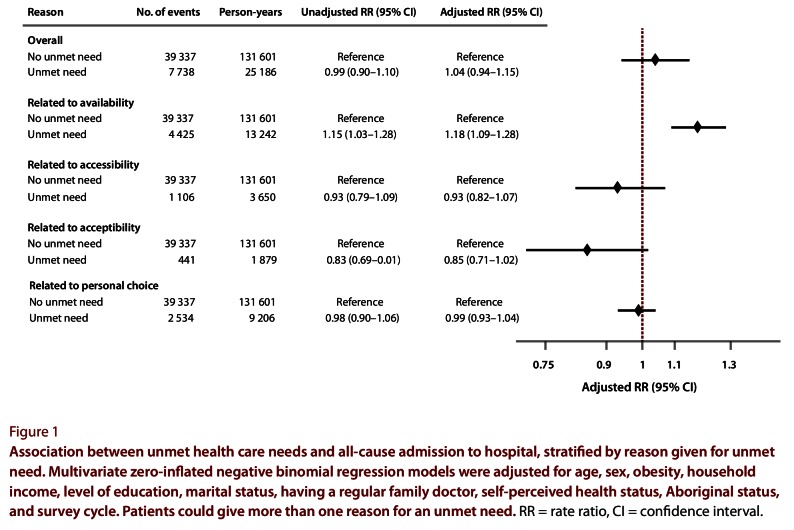
Results: Of the 51 932 adults with self-reported chronic disease, 15.5% reported an unmet health care need. Participants with unmet health care needs had a risk of all-cause admission to hospital similar to that of patients with no unmet needs (adjusted rate ratio [RR] 1.04, 95% confidence interval [CI] 0.94-1.15). When stratified by type of need, participants who reported issues of limited resource availability had a slightly higher risk of hospital admission (RR 1.18, 95% CI 1.09-1.28). There was no association between unmet needs and length of stay, readmission, or in-hospital death.
Interpretation: Overall, unmet health care needs were not associated with an increased risk of admission to hospital among those with chronic conditions. However, certain types of unmet needs may be associated with higher or lower risk. Whether unmet needs are associated with other measures of resource use remains to be determined.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


