Byron R Spencer, Omar M Khan, Bentley J Bobrow, Bart M Demaerschalk
{"title":"在初级卒中中心接受溶栓治疗的急性缺血性卒中患者的紧急医疗服务支持。","authors":"Byron R Spencer, Omar M Khan, Bentley J Bobrow, Bart M Demaerschalk","doi":"10.4137/jcnsd.s2221","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Emergency Medical Services (EMS) is a vital link in the overall chain of stroke survival. A Primary Stroke Center (PSC) relies heavily on the 9-1-1 response system along with the ability of EMS personnel to accurately diagnose acute stroke. Other critical elements include identifying time of symptom onset, providing pre-hospital care, selecting a destination PSC, and communicating estimated time of arrival (ETA).</p><p><strong>Purpose: </strong>Our purpose was to evaluate the EMS component of thrombolysed acute ischemic stroke patient care at our PSC.</p><p><strong>Methods: </strong>In a retrospective manner we retrieved electronic copies of the EMS incident reports for every thrombolysed ischemic stroke patient treated at our PSC from September 2001 to August 2005. The following data elements were extracted: location of victim, EMS agency, times of dispatch, scene, departure, emergency department (ED) arrival, recordings of time of stroke onset, blood pressure (BP), heart rate (HR), cardiac rhythm, blood glucose (BG), Glasgow Coma Scale (GCS), Cincinnati Stroke Scale (CSS) elements, emergency medical personnel field assessment, and transport decision making.</p><p><strong>Results: </strong>Eighty acute ischemic stroke patients received thrombolysis during the study interval. Eighty-one percent arrived by EMS. Two EMS agencies transported to our PSC. Mean dispatch-to-scene time was 6 min, on-scene time was 16 min, transport time was 10 min. Stroke onset time was recorded in 68%, BP, HR, and cardiac rhythm each in 100%, BG in 81%, GCS in 100%, CSS in 100%, and acute stroke diagnosis was made in 88%. Various diagnostic terms were employed: cerebrovascular accident in 40%, unilateral weakness or numbness in 20%, loss of consciousness in 16%, stroke in 8%, other stroke terms in 4%. In 87% of incident reports there was documentation of decision-making to transport to the nearest PSC in conjunction with pre-notification.</p><p><strong>Conclusion: </strong>The EMS component of thrombolysed acute ischemic stroke patients care at our PSC appeared to be very good overall. Diagnostic accuracy was excellent, field assessment, decision-making, and transport times were very good. There was still room for improvement in documentation of stroke onset and in employment of a common term for acute stroke.</p>","PeriodicalId":89798,"journal":{"name":"Journal of brain disease","volume":"1 ","pages":"13-7"},"PeriodicalIF":0.0000,"publicationDate":"2009-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4137/jcnsd.s2221","citationCount":"4","resultStr":"{\"title\":\"Emergency medical services support for acute ischemic stroke patients receiving thrombolysis at a primary stroke center.\",\"authors\":\"Byron R Spencer, Omar M Khan, Bentley J Bobrow, Bart M Demaerschalk\",\"doi\":\"10.4137/jcnsd.s2221\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Emergency Medical Services (EMS) is a vital link in the overall chain of stroke survival. A Primary Stroke Center (PSC) relies heavily on the 9-1-1 response system along with the ability of EMS personnel to accurately diagnose acute stroke. Other critical elements include identifying time of symptom onset, providing pre-hospital care, selecting a destination PSC, and communicating estimated time of arrival (ETA).</p><p><strong>Purpose: </strong>Our purpose was to evaluate the EMS component of thrombolysed acute ischemic stroke patient care at our PSC.</p><p><strong>Methods: </strong>In a retrospective manner we retrieved electronic copies of the EMS incident reports for every thrombolysed ischemic stroke patient treated at our PSC from September 2001 to August 2005. The following data elements were extracted: location of victim, EMS agency, times of dispatch, scene, departure, emergency department (ED) arrival, recordings of time of stroke onset, blood pressure (BP), heart rate (HR), cardiac rhythm, blood glucose (BG), Glasgow Coma Scale (GCS), Cincinnati Stroke Scale (CSS) elements, emergency medical personnel field assessment, and transport decision making.</p><p><strong>Results: </strong>Eighty acute ischemic stroke patients received thrombolysis during the study interval. Eighty-one percent arrived by EMS. Two EMS agencies transported to our PSC. Mean dispatch-to-scene time was 6 min, on-scene time was 16 min, transport time was 10 min. Stroke onset time was recorded in 68%, BP, HR, and cardiac rhythm each in 100%, BG in 81%, GCS in 100%, CSS in 100%, and acute stroke diagnosis was made in 88%. Various diagnostic terms were employed: cerebrovascular accident in 40%, unilateral weakness or numbness in 20%, loss of consciousness in 16%, stroke in 8%, other stroke terms in 4%. In 87% of incident reports there was documentation of decision-making to transport to the nearest PSC in conjunction with pre-notification.</p><p><strong>Conclusion: </strong>The EMS component of thrombolysed acute ischemic stroke patients care at our PSC appeared to be very good overall. Diagnostic accuracy was excellent, field assessment, decision-making, and transport times were very good. There was still room for improvement in documentation of stroke onset and in employment of a common term for acute stroke.</p>\",\"PeriodicalId\":89798,\"journal\":{\"name\":\"Journal of brain disease\",\"volume\":\"1 \",\"pages\":\"13-7\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2009-03-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.4137/jcnsd.s2221\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of brain disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4137/jcnsd.s2221\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2009/1/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of brain disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4137/jcnsd.s2221","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2009/1/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
Emergency medical services support for acute ischemic stroke patients receiving thrombolysis at a primary stroke center.
Background: Emergency Medical Services (EMS) is a vital link in the overall chain of stroke survival. A Primary Stroke Center (PSC) relies heavily on the 9-1-1 response system along with the ability of EMS personnel to accurately diagnose acute stroke. Other critical elements include identifying time of symptom onset, providing pre-hospital care, selecting a destination PSC, and communicating estimated time of arrival (ETA).
Purpose: Our purpose was to evaluate the EMS component of thrombolysed acute ischemic stroke patient care at our PSC.
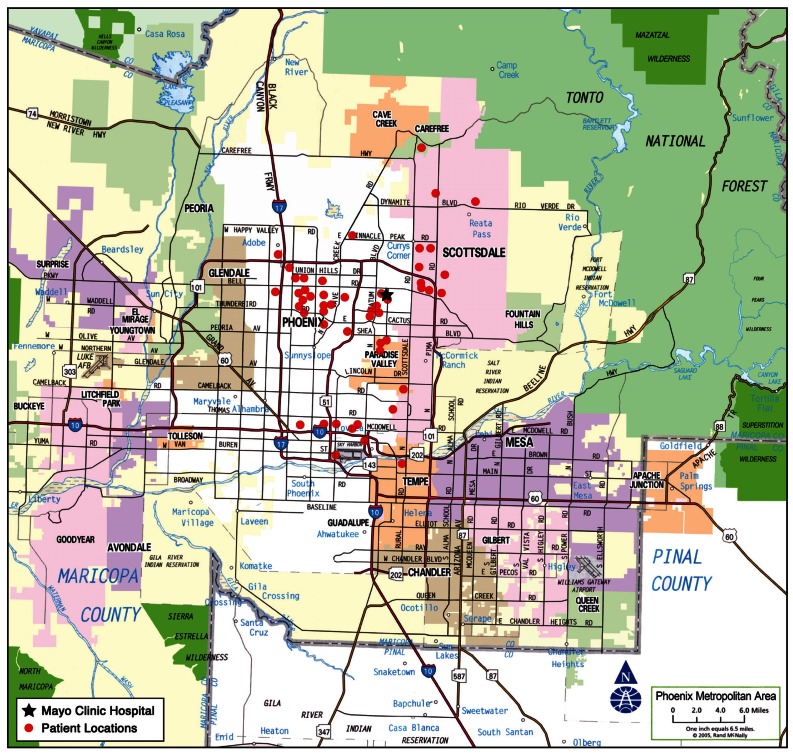
Methods: In a retrospective manner we retrieved electronic copies of the EMS incident reports for every thrombolysed ischemic stroke patient treated at our PSC from September 2001 to August 2005. The following data elements were extracted: location of victim, EMS agency, times of dispatch, scene, departure, emergency department (ED) arrival, recordings of time of stroke onset, blood pressure (BP), heart rate (HR), cardiac rhythm, blood glucose (BG), Glasgow Coma Scale (GCS), Cincinnati Stroke Scale (CSS) elements, emergency medical personnel field assessment, and transport decision making.
Results: Eighty acute ischemic stroke patients received thrombolysis during the study interval. Eighty-one percent arrived by EMS. Two EMS agencies transported to our PSC. Mean dispatch-to-scene time was 6 min, on-scene time was 16 min, transport time was 10 min. Stroke onset time was recorded in 68%, BP, HR, and cardiac rhythm each in 100%, BG in 81%, GCS in 100%, CSS in 100%, and acute stroke diagnosis was made in 88%. Various diagnostic terms were employed: cerebrovascular accident in 40%, unilateral weakness or numbness in 20%, loss of consciousness in 16%, stroke in 8%, other stroke terms in 4%. In 87% of incident reports there was documentation of decision-making to transport to the nearest PSC in conjunction with pre-notification.
Conclusion: The EMS component of thrombolysed acute ischemic stroke patients care at our PSC appeared to be very good overall. Diagnostic accuracy was excellent, field assessment, decision-making, and transport times were very good. There was still room for improvement in documentation of stroke onset and in employment of a common term for acute stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


