{"title":"原发性骨髓纤维化和髓外母细胞转化伴噬血细胞增多。","authors":"Misung Kim, Jooryung Huh","doi":"10.5045/kjh.2012.47.4.244","DOIUrl":null,"url":null,"abstract":"which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A 72-year-old woman presented with bleeding, swollen gums, and painful cervical lymphadenopathy. A CT scan revealed diffuse lymphadenopathy and hepatosplenomegaly. Initial laboratory tests showed the following: WBC level, 11.1 μg/mL; and a differential count with marked leukocytosis with a left shift. Bone marrow biopsy indicated prefibrotic myelofibrosis. There was no evidence of JAK2 or BCR/ABL mutation or Epstein-Barr virus load. Trisomy 8 mosaicism was detected (47, XY, +8[6]/46, XY[24]) on karyotyping. Excisional lymph node biopsy revealed immature myeloid cells admixed with mature myeloid components and occasional megakaryocytes (A: H&E, ×400). Most notably, there were numerous hemophagocytic macrophages (arrowheads). Blasts comprised 40% of the total cellularity and showed a mixture of strongly MPO-positive myeloblasts and MPO-negative, CD68-positive, and CD163-positive monoblastic cells. The patient was diagnosed with primary myelofibrosis and extramedullary blastic transformation (granulocytic sarcoma) with acute myelomonoblastic differentiation accompanied by hemophago-cytosis. Therefore, hydroxyurea chemotherapy was initiated. Hemophagocytosis can be seen in leukemic transformation of myelofibrosis.","PeriodicalId":23001,"journal":{"name":"The Korean Journal of Hematology","volume":"47 4","pages":"244"},"PeriodicalIF":0.0000,"publicationDate":"2012-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5045/kjh.2012.47.4.244","citationCount":"2","resultStr":"{\"title\":\"Primary myelofibrosis and extramedullary blastic transformation with hemophagocytosis.\",\"authors\":\"Misung Kim, Jooryung Huh\",\"doi\":\"10.5045/kjh.2012.47.4.244\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A 72-year-old woman presented with bleeding, swollen gums, and painful cervical lymphadenopathy. A CT scan revealed diffuse lymphadenopathy and hepatosplenomegaly. Initial laboratory tests showed the following: WBC level, 11.1 μg/mL; and a differential count with marked leukocytosis with a left shift. Bone marrow biopsy indicated prefibrotic myelofibrosis. There was no evidence of JAK2 or BCR/ABL mutation or Epstein-Barr virus load. Trisomy 8 mosaicism was detected (47, XY, +8[6]/46, XY[24]) on karyotyping. Excisional lymph node biopsy revealed immature myeloid cells admixed with mature myeloid components and occasional megakaryocytes (A: H&E, ×400). Most notably, there were numerous hemophagocytic macrophages (arrowheads). Blasts comprised 40% of the total cellularity and showed a mixture of strongly MPO-positive myeloblasts and MPO-negative, CD68-positive, and CD163-positive monoblastic cells. The patient was diagnosed with primary myelofibrosis and extramedullary blastic transformation (granulocytic sarcoma) with acute myelomonoblastic differentiation accompanied by hemophago-cytosis. Therefore, hydroxyurea chemotherapy was initiated. Hemophagocytosis can be seen in leukemic transformation of myelofibrosis.\",\"PeriodicalId\":23001,\"journal\":{\"name\":\"The Korean Journal of Hematology\",\"volume\":\"47 4\",\"pages\":\"244\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2012-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.5045/kjh.2012.47.4.244\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Korean Journal of Hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5045/kjh.2012.47.4.244\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2012/12/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/kjh.2012.47.4.244","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/12/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Primary myelofibrosis and extramedullary blastic transformation with hemophagocytosis.
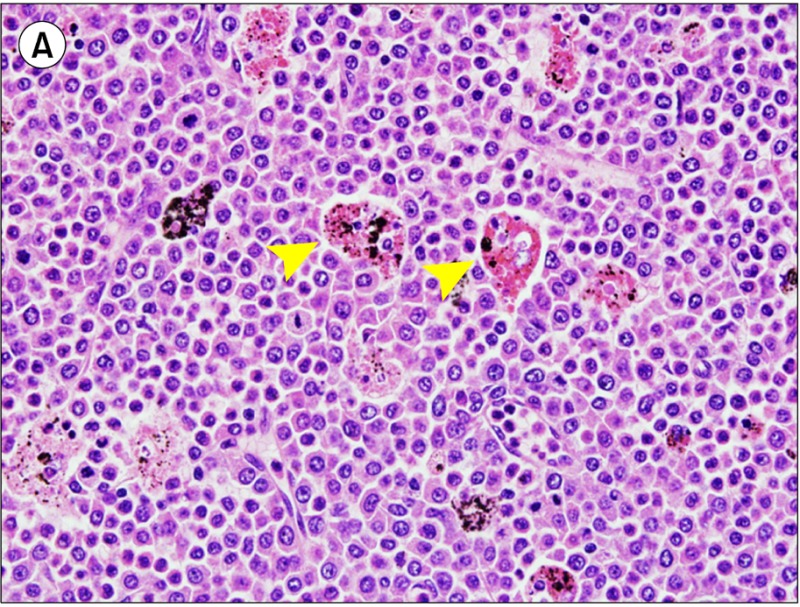
which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A 72-year-old woman presented with bleeding, swollen gums, and painful cervical lymphadenopathy. A CT scan revealed diffuse lymphadenopathy and hepatosplenomegaly. Initial laboratory tests showed the following: WBC level, 11.1 μg/mL; and a differential count with marked leukocytosis with a left shift. Bone marrow biopsy indicated prefibrotic myelofibrosis. There was no evidence of JAK2 or BCR/ABL mutation or Epstein-Barr virus load. Trisomy 8 mosaicism was detected (47, XY, +8[6]/46, XY[24]) on karyotyping. Excisional lymph node biopsy revealed immature myeloid cells admixed with mature myeloid components and occasional megakaryocytes (A: H&E, ×400). Most notably, there were numerous hemophagocytic macrophages (arrowheads). Blasts comprised 40% of the total cellularity and showed a mixture of strongly MPO-positive myeloblasts and MPO-negative, CD68-positive, and CD163-positive monoblastic cells. The patient was diagnosed with primary myelofibrosis and extramedullary blastic transformation (granulocytic sarcoma) with acute myelomonoblastic differentiation accompanied by hemophago-cytosis. Therefore, hydroxyurea chemotherapy was initiated. Hemophagocytosis can be seen in leukemic transformation of myelofibrosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


