Laith H Jamil, Ana M Chindris, Kanwar R S Gill, Daniela Scimeca, John A Stauffer, Michael G Heckman, Shon E Meek, Justin H Nguyen, Horacio J Asbun, Massimo Raimondo, Timothy A Woodward, Michael B Wallace
{"title":"导管内乳头状粘液瘤全胰切除术后血糖控制:一项探索性研究。","authors":"Laith H Jamil, Ana M Chindris, Kanwar R S Gill, Daniela Scimeca, John A Stauffer, Michael G Heckman, Shon E Meek, Justin H Nguyen, Horacio J Asbun, Massimo Raimondo, Timothy A Woodward, Michael B Wallace","doi":"10.1155/2012/381328","DOIUrl":null,"url":null,"abstract":"<p><p>Background. Glycemic control following total pancreatectomy (TP) has been thought to be difficult to manage. Diffuse intraductal papillary mucinous neoplasm (IPMN) is a potentially curable precursor to pancreatic adenocarcinoma, best treated by TP. Objective. Compare glycemic control in patients undergoing TP for IPMN to patients with type 1 diabetes mellitus (DM). Design/Setting. Retrospective cohort. Outcome Measure. Hemoglobin A1C(HbA1C) at 6, 12, 18, and 24 months after TP. In the control group, baseline was defined as 6 months prior to the first HbA1c measure. Results. Mean HgbA1C at each point of interest was similar between TP and type I DM patients (6 months (7.5% versus 7.7%, P = 0.52), 12 months (7.3% versus 8.0%, P = 0.081), 18 months (7.7% and 7.6%, P = 0.64), and at 24 months (7.3% versus 7.8%, P = 0.10)). Seven TP patients (50%) experienced a hypoglycemic event compared to 65 type 1 DM patients (65%, P = 0.38). Limitations. Small number of TP patients, retrospective design, lack of long-termfollowup. Conclusion. This suggests that glycemic control following TP for IPMNcan be well managed, similar to type 1 DM patients. Fear of DM following TP for IPMN should not preclude surgery when TP is indicated.</p>","PeriodicalId":77165,"journal":{"name":"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery","volume":"2012 ","pages":"381328"},"PeriodicalIF":0.0000,"publicationDate":"2012-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2012/381328","citationCount":"27","resultStr":"{\"title\":\"Glycemic control after total pancreatectomy for intraductal papillary mucinous neoplasm: an exploratory study.\",\"authors\":\"Laith H Jamil, Ana M Chindris, Kanwar R S Gill, Daniela Scimeca, John A Stauffer, Michael G Heckman, Shon E Meek, Justin H Nguyen, Horacio J Asbun, Massimo Raimondo, Timothy A Woodward, Michael B Wallace\",\"doi\":\"10.1155/2012/381328\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Background. Glycemic control following total pancreatectomy (TP) has been thought to be difficult to manage. Diffuse intraductal papillary mucinous neoplasm (IPMN) is a potentially curable precursor to pancreatic adenocarcinoma, best treated by TP. Objective. Compare glycemic control in patients undergoing TP for IPMN to patients with type 1 diabetes mellitus (DM). Design/Setting. Retrospective cohort. Outcome Measure. Hemoglobin A1C(HbA1C) at 6, 12, 18, and 24 months after TP. In the control group, baseline was defined as 6 months prior to the first HbA1c measure. Results. Mean HgbA1C at each point of interest was similar between TP and type I DM patients (6 months (7.5% versus 7.7%, P = 0.52), 12 months (7.3% versus 8.0%, P = 0.081), 18 months (7.7% and 7.6%, P = 0.64), and at 24 months (7.3% versus 7.8%, P = 0.10)). Seven TP patients (50%) experienced a hypoglycemic event compared to 65 type 1 DM patients (65%, P = 0.38). Limitations. Small number of TP patients, retrospective design, lack of long-termfollowup. Conclusion. This suggests that glycemic control following TP for IPMNcan be well managed, similar to type 1 DM patients. Fear of DM following TP for IPMN should not preclude surgery when TP is indicated.</p>\",\"PeriodicalId\":77165,\"journal\":{\"name\":\"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery\",\"volume\":\"2012 \",\"pages\":\"381328\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2012-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2012/381328\",\"citationCount\":\"27\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2012/381328\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2012/8/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2012/381328","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/8/26 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Glycemic control after total pancreatectomy for intraductal papillary mucinous neoplasm: an exploratory study.
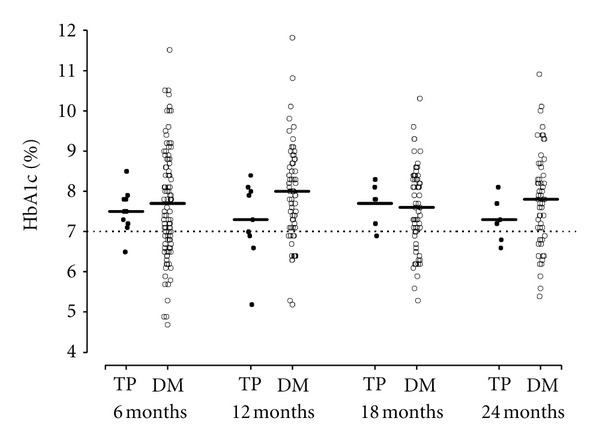
Background. Glycemic control following total pancreatectomy (TP) has been thought to be difficult to manage. Diffuse intraductal papillary mucinous neoplasm (IPMN) is a potentially curable precursor to pancreatic adenocarcinoma, best treated by TP. Objective. Compare glycemic control in patients undergoing TP for IPMN to patients with type 1 diabetes mellitus (DM). Design/Setting. Retrospective cohort. Outcome Measure. Hemoglobin A1C(HbA1C) at 6, 12, 18, and 24 months after TP. In the control group, baseline was defined as 6 months prior to the first HbA1c measure. Results. Mean HgbA1C at each point of interest was similar between TP and type I DM patients (6 months (7.5% versus 7.7%, P = 0.52), 12 months (7.3% versus 8.0%, P = 0.081), 18 months (7.7% and 7.6%, P = 0.64), and at 24 months (7.3% versus 7.8%, P = 0.10)). Seven TP patients (50%) experienced a hypoglycemic event compared to 65 type 1 DM patients (65%, P = 0.38). Limitations. Small number of TP patients, retrospective design, lack of long-termfollowup. Conclusion. This suggests that glycemic control following TP for IPMNcan be well managed, similar to type 1 DM patients. Fear of DM following TP for IPMN should not preclude surgery when TP is indicated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


