Hye Jin Oh, Myung Jae Yun, Seong Tae Lee, Seung June Lee, So Yeon Oh, In Sohn
{"title":"长期桥本甲状腺炎和利妥昔单抗成功治疗后的Evans综合征。","authors":"Hye Jin Oh, Myung Jae Yun, Seong Tae Lee, Seung June Lee, So Yeon Oh, In Sohn","doi":"10.5045/kjh.2011.46.4.279","DOIUrl":null,"url":null,"abstract":"<p><p>We report a case of a 51-year-old woman with Evans syndrome (autoimmune hemolytic anemia and primary immune thrombocytopenia) and hypothyroidism. She was previously diagnosed with Hashimoto's thyroiditis in 1994 (age, 35) and autoimmune hemolytic anemia (AIHA) 3 years ago. She was treated with oral prednisolone. After a period, in which the anemia waxed and waned, there was an abrupt development of thrombocytopenia (nadir 15×10(9)/L) that coincided with the tapering off of prednisolone after 3 years of administration. Because her thrombocytopenia was refractory to prednisolone, we administered rituximab (375 mg/m(2) weekly) for 4 weeks. Two weeks after the completion of the rituximab treatment, her platelet count was up to 92×10(9)/L. No intermittent peaking of thyroid stimulating hormone occurred after rituximab treatment was initiated. Evans syndrome and autoimmune thyroiditis might share common pathophysiological mechanisms. This notion supports the use of rituximab in a patient suffering from these disorders.</p>","PeriodicalId":23001,"journal":{"name":"The Korean Journal of Hematology","volume":"46 4","pages":"279-82"},"PeriodicalIF":0.0000,"publicationDate":"2011-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5045/kjh.2011.46.4.279","citationCount":"13","resultStr":"{\"title\":\"Evans syndrome following long-standing Hashimoto's thyroiditis and successful treatment with rituximab.\",\"authors\":\"Hye Jin Oh, Myung Jae Yun, Seong Tae Lee, Seung June Lee, So Yeon Oh, In Sohn\",\"doi\":\"10.5045/kjh.2011.46.4.279\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We report a case of a 51-year-old woman with Evans syndrome (autoimmune hemolytic anemia and primary immune thrombocytopenia) and hypothyroidism. She was previously diagnosed with Hashimoto's thyroiditis in 1994 (age, 35) and autoimmune hemolytic anemia (AIHA) 3 years ago. She was treated with oral prednisolone. After a period, in which the anemia waxed and waned, there was an abrupt development of thrombocytopenia (nadir 15×10(9)/L) that coincided with the tapering off of prednisolone after 3 years of administration. Because her thrombocytopenia was refractory to prednisolone, we administered rituximab (375 mg/m(2) weekly) for 4 weeks. Two weeks after the completion of the rituximab treatment, her platelet count was up to 92×10(9)/L. No intermittent peaking of thyroid stimulating hormone occurred after rituximab treatment was initiated. Evans syndrome and autoimmune thyroiditis might share common pathophysiological mechanisms. This notion supports the use of rituximab in a patient suffering from these disorders.</p>\",\"PeriodicalId\":23001,\"journal\":{\"name\":\"The Korean Journal of Hematology\",\"volume\":\"46 4\",\"pages\":\"279-82\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.5045/kjh.2011.46.4.279\",\"citationCount\":\"13\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Korean Journal of Hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5045/kjh.2011.46.4.279\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2011/12/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/kjh.2011.46.4.279","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2011/12/27 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Evans syndrome following long-standing Hashimoto's thyroiditis and successful treatment with rituximab.
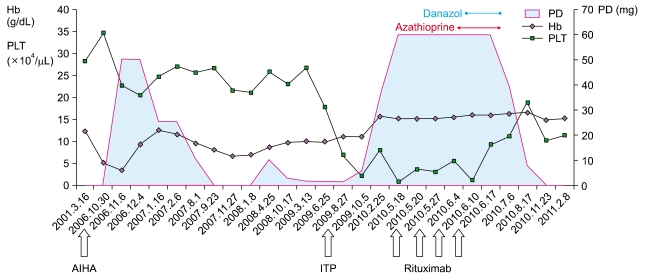
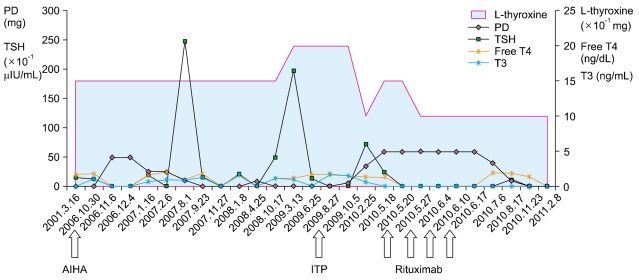
We report a case of a 51-year-old woman with Evans syndrome (autoimmune hemolytic anemia and primary immune thrombocytopenia) and hypothyroidism. She was previously diagnosed with Hashimoto's thyroiditis in 1994 (age, 35) and autoimmune hemolytic anemia (AIHA) 3 years ago. She was treated with oral prednisolone. After a period, in which the anemia waxed and waned, there was an abrupt development of thrombocytopenia (nadir 15×10(9)/L) that coincided with the tapering off of prednisolone after 3 years of administration. Because her thrombocytopenia was refractory to prednisolone, we administered rituximab (375 mg/m(2) weekly) for 4 weeks. Two weeks after the completion of the rituximab treatment, her platelet count was up to 92×10(9)/L. No intermittent peaking of thyroid stimulating hormone occurred after rituximab treatment was initiated. Evans syndrome and autoimmune thyroiditis might share common pathophysiological mechanisms. This notion supports the use of rituximab in a patient suffering from these disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


