{"title":"通过细针穿刺细胞学诊断hiv相关的浆母细胞淋巴瘤。","authors":"Michele Bibas, Andrea Baiocchini","doi":"10.5045/kjh.2011.46.4.214","DOIUrl":null,"url":null,"abstract":"which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A 25-year-old man without any relevant medical history was admitted to our hospital for progressive weakness, fever, night sweats, and weight loss. Physical examination showed several round skin nodules and multiple painless lymph nodes in the axillary and inguinal regions (A). A CT scan revealed diffuse lymphadenopathy and hepatosplenomegaly with multiple liver nodules (B). Percutaneous fine-needle aspiration cytology (FNAC) of a skin nodule revealed large atypical cells with plasmacytoid and anaplastic features, which indicated a lymphoma (C). The diagnosis of plasmablastic lymphoma was confirmed by traditional biopsy of another cutaneous lesion (D). Neoplastic cells were strongly positive (>95%) for CD138, CD43, and Ki-67, and were negative for CD3, CD20, CD45, MUM-1, EBV, and HHV8. Because this type of lymphoma is mainly associated with HIV, blood samples were tested for HIV antibodies. The HIV RNA load was 389.98 cp/mL, and CD4 + cell count was 76/mm 3. The patient was diagnosed with HIV-associated disseminated extraoral plasmablastic lymphoma. Cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) chemotherapy was initiated for the lymphoma and highly active antiretroviral therapy (HAART) for HIV infection.","PeriodicalId":23001,"journal":{"name":"The Korean Journal of Hematology","volume":"46 4","pages":"214"},"PeriodicalIF":0.0000,"publicationDate":"2011-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5045/kjh.2011.46.4.214","citationCount":"1","resultStr":"{\"title\":\"HIV-associated plasmablastic lymphoma diagnosed by fine-needle aspiration cytology.\",\"authors\":\"Michele Bibas, Andrea Baiocchini\",\"doi\":\"10.5045/kjh.2011.46.4.214\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A 25-year-old man without any relevant medical history was admitted to our hospital for progressive weakness, fever, night sweats, and weight loss. Physical examination showed several round skin nodules and multiple painless lymph nodes in the axillary and inguinal regions (A). A CT scan revealed diffuse lymphadenopathy and hepatosplenomegaly with multiple liver nodules (B). Percutaneous fine-needle aspiration cytology (FNAC) of a skin nodule revealed large atypical cells with plasmacytoid and anaplastic features, which indicated a lymphoma (C). The diagnosis of plasmablastic lymphoma was confirmed by traditional biopsy of another cutaneous lesion (D). Neoplastic cells were strongly positive (>95%) for CD138, CD43, and Ki-67, and were negative for CD3, CD20, CD45, MUM-1, EBV, and HHV8. Because this type of lymphoma is mainly associated with HIV, blood samples were tested for HIV antibodies. The HIV RNA load was 389.98 cp/mL, and CD4 + cell count was 76/mm 3. The patient was diagnosed with HIV-associated disseminated extraoral plasmablastic lymphoma. Cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) chemotherapy was initiated for the lymphoma and highly active antiretroviral therapy (HAART) for HIV infection.\",\"PeriodicalId\":23001,\"journal\":{\"name\":\"The Korean Journal of Hematology\",\"volume\":\"46 4\",\"pages\":\"214\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.5045/kjh.2011.46.4.214\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Korean Journal of Hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5045/kjh.2011.46.4.214\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2011/12/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/kjh.2011.46.4.214","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2011/12/27 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
HIV-associated plasmablastic lymphoma diagnosed by fine-needle aspiration cytology.
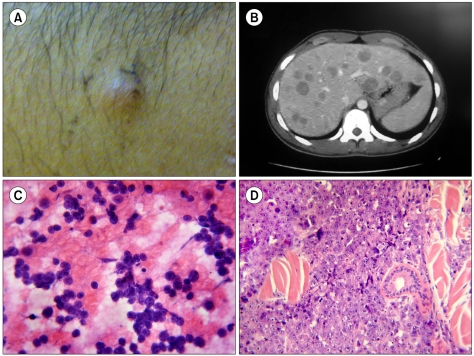
which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A 25-year-old man without any relevant medical history was admitted to our hospital for progressive weakness, fever, night sweats, and weight loss. Physical examination showed several round skin nodules and multiple painless lymph nodes in the axillary and inguinal regions (A). A CT scan revealed diffuse lymphadenopathy and hepatosplenomegaly with multiple liver nodules (B). Percutaneous fine-needle aspiration cytology (FNAC) of a skin nodule revealed large atypical cells with plasmacytoid and anaplastic features, which indicated a lymphoma (C). The diagnosis of plasmablastic lymphoma was confirmed by traditional biopsy of another cutaneous lesion (D). Neoplastic cells were strongly positive (>95%) for CD138, CD43, and Ki-67, and were negative for CD3, CD20, CD45, MUM-1, EBV, and HHV8. Because this type of lymphoma is mainly associated with HIV, blood samples were tested for HIV antibodies. The HIV RNA load was 389.98 cp/mL, and CD4 + cell count was 76/mm 3. The patient was diagnosed with HIV-associated disseminated extraoral plasmablastic lymphoma. Cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) chemotherapy was initiated for the lymphoma and highly active antiretroviral therapy (HAART) for HIV infection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


