{"title":"为下一个澳大利亚卫生保健协议制定“强有力的绩效基准”:需要一个新的框架。","authors":"Stephen J Duckett, Michael Ward","doi":"10.1186/1743-8462-5-1","DOIUrl":null,"url":null,"abstract":"<p><p> If the outcomes of the recent COAG meeting are implemented, Australia will have a new set of benchmarks for its health system within a few months. This is a non-trivial task. Choice of benchmarks will, explicitly or implicitly, reflect a framework about how the health system works, what is important or to be valued and how the benchmarks are to be used. In this article we argue that the health system is dynamic and so benchmarks need to measure flows and interfaces rather than simply cross-sectional or static performance. We also argue that benchmarks need to be developed taking into account three perspectives: patient, clinician and funder. Each of these perspectives is critical and good performance from one perspective or on one dimension doesn't imply good performance on either (or both) of the others.The three perspectives (we term the dimensions patient assessed value, performance on clinical interventions and efficiency) can each be decomposed into a number of elements. For example, patient assessed value is influenced by timeliness, cost to the patient, the extent to which their expectations are met, the way they are treated and the extent to which there is continuity of care.We also argue that the way information is presented is important: cross sectional, dated measures provide much less information and are much less useful than approaches based on statistical process control. The latter also focuses attention on improvement and trends, encouraging action rather than simply blame of poorer performers.</p>","PeriodicalId":87170,"journal":{"name":"Australia and New Zealand health policy","volume":"5 ","pages":"1"},"PeriodicalIF":0.0000,"publicationDate":"2008-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1743-8462-5-1","citationCount":"0","resultStr":"{\"title\":\"Developing 'robust performance benchmarks' for the next Australian Health Care Agreement: the need for a new framework.\",\"authors\":\"Stephen J Duckett, Michael Ward\",\"doi\":\"10.1186/1743-8462-5-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p> If the outcomes of the recent COAG meeting are implemented, Australia will have a new set of benchmarks for its health system within a few months. This is a non-trivial task. Choice of benchmarks will, explicitly or implicitly, reflect a framework about how the health system works, what is important or to be valued and how the benchmarks are to be used. In this article we argue that the health system is dynamic and so benchmarks need to measure flows and interfaces rather than simply cross-sectional or static performance. We also argue that benchmarks need to be developed taking into account three perspectives: patient, clinician and funder. Each of these perspectives is critical and good performance from one perspective or on one dimension doesn't imply good performance on either (or both) of the others.The three perspectives (we term the dimensions patient assessed value, performance on clinical interventions and efficiency) can each be decomposed into a number of elements. For example, patient assessed value is influenced by timeliness, cost to the patient, the extent to which their expectations are met, the way they are treated and the extent to which there is continuity of care.We also argue that the way information is presented is important: cross sectional, dated measures provide much less information and are much less useful than approaches based on statistical process control. The latter also focuses attention on improvement and trends, encouraging action rather than simply blame of poorer performers.</p>\",\"PeriodicalId\":87170,\"journal\":{\"name\":\"Australia and New Zealand health policy\",\"volume\":\"5 \",\"pages\":\"1\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2008-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/1743-8462-5-1\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Australia and New Zealand health policy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/1743-8462-5-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Australia and New Zealand health policy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1743-8462-5-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Developing 'robust performance benchmarks' for the next Australian Health Care Agreement: the need for a new framework.
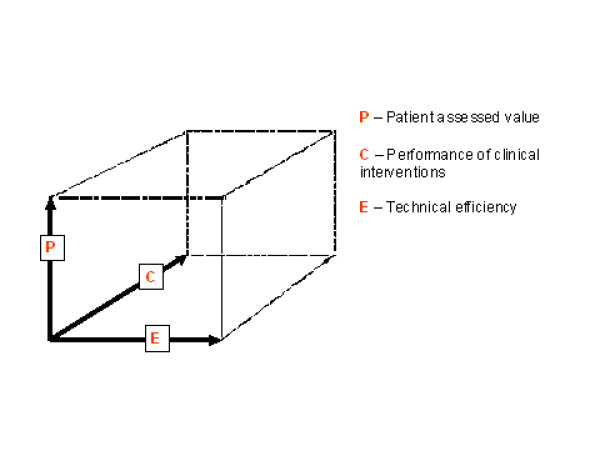
If the outcomes of the recent COAG meeting are implemented, Australia will have a new set of benchmarks for its health system within a few months. This is a non-trivial task. Choice of benchmarks will, explicitly or implicitly, reflect a framework about how the health system works, what is important or to be valued and how the benchmarks are to be used. In this article we argue that the health system is dynamic and so benchmarks need to measure flows and interfaces rather than simply cross-sectional or static performance. We also argue that benchmarks need to be developed taking into account three perspectives: patient, clinician and funder. Each of these perspectives is critical and good performance from one perspective or on one dimension doesn't imply good performance on either (or both) of the others.The three perspectives (we term the dimensions patient assessed value, performance on clinical interventions and efficiency) can each be decomposed into a number of elements. For example, patient assessed value is influenced by timeliness, cost to the patient, the extent to which their expectations are met, the way they are treated and the extent to which there is continuity of care.We also argue that the way information is presented is important: cross sectional, dated measures provide much less information and are much less useful than approaches based on statistical process control. The latter also focuses attention on improvement and trends, encouraging action rather than simply blame of poorer performers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


