Moses R Kamya, Adoke Yeka, Hasifa Bukirwa, Myers Lugemwa, John B Rwakimari, Sarah G Staedke, Ambrose O Talisuna, Bryan Greenhouse, François Nosten, Philip J Rosenthal, Fred Wabwire-Mangen, Grant Dorsey
{"title":"青蒿素-氨芳汀与双氢青蒿素-哌喹治疗疟疾:一项随机试验","authors":"Moses R Kamya, Adoke Yeka, Hasifa Bukirwa, Myers Lugemwa, John B Rwakimari, Sarah G Staedke, Ambrose O Talisuna, Bryan Greenhouse, François Nosten, Philip J Rosenthal, Fred Wabwire-Mangen, Grant Dorsey","doi":"10.1371/journal.pctr.0020020","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To compare the efficacy and safety of artemether-lumefantrine (AL) and dihydroartemisinin-piperaquine (DP) for treating uncomplicated falciparum malaria in Uganda.</p><p><strong>Design: </strong>Randomized single-blinded clinical trial.</p><p><strong>Setting: </strong>Apac, Uganda, an area of very high malaria transmission intensity.</p><p><strong>Participants: </strong>Children aged 6 mo to 10 y with uncomplicated falciparum malaria.</p><p><strong>Intervention: </strong>Treatment of malaria with AL or DP, each following standard 3-d dosing regimens.</p><p><strong>Outcome measures: </strong>Risks of recurrent parasitemia at 28 and 42 d, unadjusted and adjusted by genotyping to distinguish recrudescences and new infections.</p><p><strong>Results: </strong>Of 421 enrolled participants, 417 (99%) completed follow-up. The unadjusted risk of recurrent falciparum parasitemia was significantly lower for participants treated with DP than for those treated with AL after 28 d (11% versus 29%; risk difference [RD] 18%, 95% confidence interval [CI] 11%-26%) and 42 d (43% versus 53%; RD 9.6%, 95% CI 0%-19%) of follow-up. Similarly, the risk of recurrent parasitemia due to possible recrudescence (adjusted by genotyping) was significantly lower for participants treated with DP than for those treated with AL after 28 d (1.9% versus 8.9%; RD 7.0%, 95% CI 2.5%-12%) and 42 d (6.9% versus 16%; RD 9.5%, 95% CI 2.8%-16%). Patients treated with DP had a lower risk of recurrent parasitemia due to non-falciparum species, development of gametocytemia, and higher mean increase in hemoglobin compared to patients treated with AL. Both drugs were well tolerated; serious adverse events were uncommon and unrelated to study drugs.</p><p><strong>Conclusion: </strong>DP was superior to AL for reducing the risk of recurrent parasitemia and gametocytemia, and provided improved hemoglobin recovery. DP thus appears to be a good alternative to AL as first-line treatment of uncomplicated malaria in Uganda. To maximize the benefit of artemisinin-based combination therapy in Africa, treatment should be integrated with aggressive strategies to reduce malaria transmission intensity.</p>","PeriodicalId":87416,"journal":{"name":"PLoS clinical trials","volume":"2 5","pages":"e20"},"PeriodicalIF":0.0000,"publicationDate":"2007-05-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1371/journal.pctr.0020020","citationCount":"159","resultStr":"{\"title\":\"Artemether-lumefantrine versus dihydroartemisinin-piperaquine for treatment of malaria: a randomized trial.\",\"authors\":\"Moses R Kamya, Adoke Yeka, Hasifa Bukirwa, Myers Lugemwa, John B Rwakimari, Sarah G Staedke, Ambrose O Talisuna, Bryan Greenhouse, François Nosten, Philip J Rosenthal, Fred Wabwire-Mangen, Grant Dorsey\",\"doi\":\"10.1371/journal.pctr.0020020\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To compare the efficacy and safety of artemether-lumefantrine (AL) and dihydroartemisinin-piperaquine (DP) for treating uncomplicated falciparum malaria in Uganda.</p><p><strong>Design: </strong>Randomized single-blinded clinical trial.</p><p><strong>Setting: </strong>Apac, Uganda, an area of very high malaria transmission intensity.</p><p><strong>Participants: </strong>Children aged 6 mo to 10 y with uncomplicated falciparum malaria.</p><p><strong>Intervention: </strong>Treatment of malaria with AL or DP, each following standard 3-d dosing regimens.</p><p><strong>Outcome measures: </strong>Risks of recurrent parasitemia at 28 and 42 d, unadjusted and adjusted by genotyping to distinguish recrudescences and new infections.</p><p><strong>Results: </strong>Of 421 enrolled participants, 417 (99%) completed follow-up. The unadjusted risk of recurrent falciparum parasitemia was significantly lower for participants treated with DP than for those treated with AL after 28 d (11% versus 29%; risk difference [RD] 18%, 95% confidence interval [CI] 11%-26%) and 42 d (43% versus 53%; RD 9.6%, 95% CI 0%-19%) of follow-up. Similarly, the risk of recurrent parasitemia due to possible recrudescence (adjusted by genotyping) was significantly lower for participants treated with DP than for those treated with AL after 28 d (1.9% versus 8.9%; RD 7.0%, 95% CI 2.5%-12%) and 42 d (6.9% versus 16%; RD 9.5%, 95% CI 2.8%-16%). Patients treated with DP had a lower risk of recurrent parasitemia due to non-falciparum species, development of gametocytemia, and higher mean increase in hemoglobin compared to patients treated with AL. Both drugs were well tolerated; serious adverse events were uncommon and unrelated to study drugs.</p><p><strong>Conclusion: </strong>DP was superior to AL for reducing the risk of recurrent parasitemia and gametocytemia, and provided improved hemoglobin recovery. DP thus appears to be a good alternative to AL as first-line treatment of uncomplicated malaria in Uganda. To maximize the benefit of artemisinin-based combination therapy in Africa, treatment should be integrated with aggressive strategies to reduce malaria transmission intensity.</p>\",\"PeriodicalId\":87416,\"journal\":{\"name\":\"PLoS clinical trials\",\"volume\":\"2 5\",\"pages\":\"e20\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2007-05-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1371/journal.pctr.0020020\",\"citationCount\":\"159\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS clinical trials\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pctr.0020020\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS clinical trials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1371/journal.pctr.0020020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 159
摘要
目的:比较青蒿素-氨芳汀(AL)和双氢青蒿素-哌喹(DP)治疗乌干达无并发症恶性疟疾的疗效和安全性。设计:随机单盲临床试验。环境:Apac,乌干达,疟疾传播强度非常高的地区。参与者:患有无并发症恶性疟疾的6个月至10岁儿童。干预:用AL或DP治疗疟疾,每一种都遵循标准的三维给药方案。结果指标:28天和42天寄生虫病复发的风险,未调整和通过基因分型调整以区分复发和新感染。结果:421名入组参与者中,417名(99%)完成随访。在28 d后,接受DP治疗的患者复发恶性寄生虫病的未调整风险显著低于接受AL治疗的患者(11% vs 29%;风险差异[RD] 18%, 95%可信区间[CI] 11%-26%)和42 d(43%对53%;RD为9.6%,95% CI为0%-19%)。同样,在28天后,接受DP治疗的患者因可能复发而复发寄生虫病的风险(通过基因分型调整)显著低于接受AL治疗的患者(1.9% vs 8.9%;RD 7.0%, 95% CI 2.5%-12%)和42 d(6.9%对16%;Rd 9.5%, 95% ci 2.8%-16%)。与AL治疗的患者相比,DP治疗的患者复发性寄生虫病的风险较低,因为非恶性疟原虫、配子体的发展和血红蛋白的平均升高。两种药物耐受性良好;严重不良事件不常见,且与研究药物无关。结论:DP在降低寄生虫病和配子细胞病复发风险方面优于AL,并能改善血红蛋白恢复。因此,在乌干达,DP似乎是AL的一个很好的替代方案,可以作为简单疟疾的一线治疗方法。为了最大限度地发挥以青蒿素为基础的联合疗法在非洲的效益,治疗应与降低疟疾传播强度的积极战略相结合。
Artemether-lumefantrine versus dihydroartemisinin-piperaquine for treatment of malaria: a randomized trial.
Objectives: To compare the efficacy and safety of artemether-lumefantrine (AL) and dihydroartemisinin-piperaquine (DP) for treating uncomplicated falciparum malaria in Uganda.
Design: Randomized single-blinded clinical trial.
Setting: Apac, Uganda, an area of very high malaria transmission intensity.
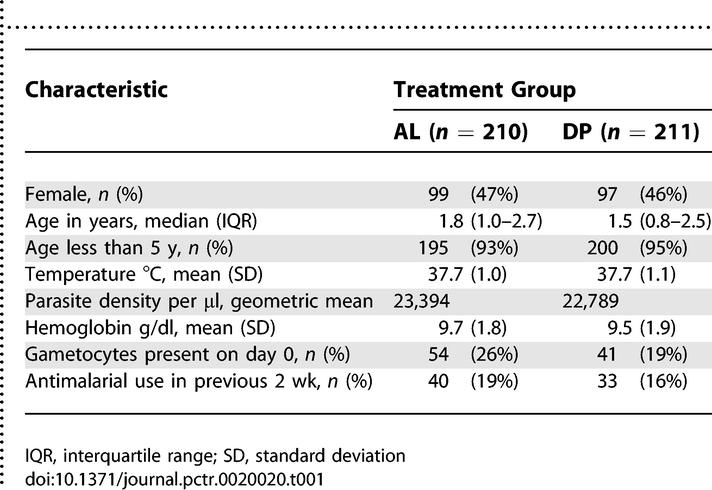
Participants: Children aged 6 mo to 10 y with uncomplicated falciparum malaria.
Intervention: Treatment of malaria with AL or DP, each following standard 3-d dosing regimens.
Outcome measures: Risks of recurrent parasitemia at 28 and 42 d, unadjusted and adjusted by genotyping to distinguish recrudescences and new infections.
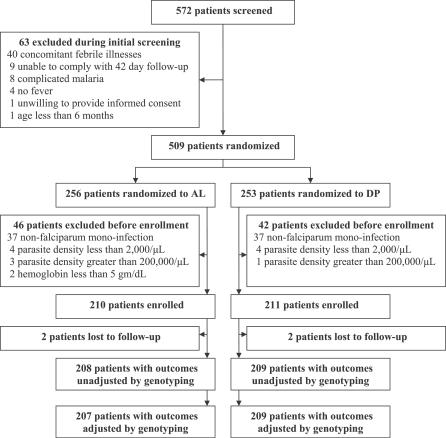
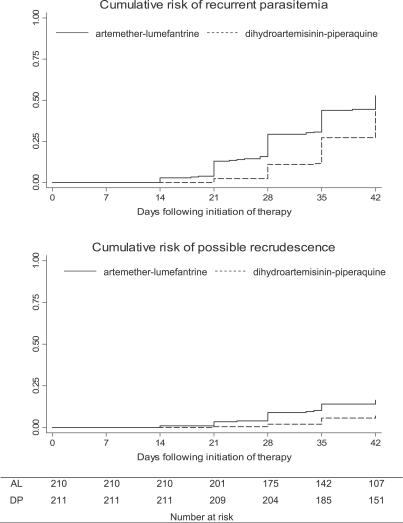
Results: Of 421 enrolled participants, 417 (99%) completed follow-up. The unadjusted risk of recurrent falciparum parasitemia was significantly lower for participants treated with DP than for those treated with AL after 28 d (11% versus 29%; risk difference [RD] 18%, 95% confidence interval [CI] 11%-26%) and 42 d (43% versus 53%; RD 9.6%, 95% CI 0%-19%) of follow-up. Similarly, the risk of recurrent parasitemia due to possible recrudescence (adjusted by genotyping) was significantly lower for participants treated with DP than for those treated with AL after 28 d (1.9% versus 8.9%; RD 7.0%, 95% CI 2.5%-12%) and 42 d (6.9% versus 16%; RD 9.5%, 95% CI 2.8%-16%). Patients treated with DP had a lower risk of recurrent parasitemia due to non-falciparum species, development of gametocytemia, and higher mean increase in hemoglobin compared to patients treated with AL. Both drugs were well tolerated; serious adverse events were uncommon and unrelated to study drugs.
Conclusion: DP was superior to AL for reducing the risk of recurrent parasitemia and gametocytemia, and provided improved hemoglobin recovery. DP thus appears to be a good alternative to AL as first-line treatment of uncomplicated malaria in Uganda. To maximize the benefit of artemisinin-based combination therapy in Africa, treatment should be integrated with aggressive strategies to reduce malaria transmission intensity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


