Jian-Yun Zhou, Xin Zhang, Hai-Bin Gao, Ze Cao, Wei Sun
{"title":"内窥镜辅助手术治疗伴有硬膜下积液的颅骨缺损。","authors":"Jian-Yun Zhou, Xin Zhang, Hai-Bin Gao, Ze Cao, Wei Sun","doi":"10.5114/wiitm.2020.99350","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Subdural effusion is a common complication that occurs after decompressive craniectomy. According to the endoscopy results, the formation mechanism of subdural effusion after decompressive craniectomy was discussed.</p><p><strong>Aim: </strong>The morphological structure of subdural effusion in skull defects was observed with endoscopy, and endoscopic-assisted surgery was performed for subdural effusion.</p><p><strong>Material and methods: </strong>From January 2018 to March 2020, 19 cases of skull repair and treatment of subdural effusion were performed. The external wall of the capsule was kept intact during the operation, subdural effusion and surgical procedure of the subdural effusion under an endoscope could be observed, and the results of endoscopic observation were described and recorded. A hemostasis gauze was placed between the two layers of the subdural effusion cavity. Another 13 cases of skull defects with subdural effusion treated without endoscopy during the same time period were enrolled in the study as the control group. The postoperative disappearance of effusion and the incidence of postoperative complications were compared between the two groups.</p><p><strong>Results: </strong>Analysis with an endoscope revealed that all cases of subdural effusion in skull defects presented capsules. The main structures included the outer wall, boundary, inner wall, and fistula. The outer wall was made up of new tissue that had formed after removing the bone flap under the skin flap by artificial peeling under the condition of keeping the whole cavity. The inner wall consisted of thickened arachnoid, dura, and artificial dura. It presented with neovascularization networks, which showed a tendency to form new membrane structures through mutual adhesion and fusion. The inner and outer wall of the skull had fused to form the boundary of the cavity. Cerebrospinal fluid fistulas were detected in 31.6% of the internal walls. Subdural effusion was effectively treated in both the experimental group and the control group. Compared with the control group, complications in the experimental group were significantly reduced.</p><p><strong>Conclusions: </strong>The effusion cavity can be divided into three types based on its structural characteristics: fistula type, membrane type, and closed type. In this study, the formation mechanism of skull defects combined with subdural effusion was explored. This represents a new method for treating subdural effusion in which hemostasis gauze is placed between the two layers of the effusion cavity and cerebrospinal fluid fistula under an endoscope, which can effectively reduce the incidence of postoperative complications.</p>","PeriodicalId":520827,"journal":{"name":"Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques","volume":" ","pages":"219-226"},"PeriodicalIF":0.0000,"publicationDate":"2021-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5114/wiitm.2020.99350","citationCount":"2","resultStr":"{\"title\":\"Endoscopic-assisted surgery for skull defects with subdural effusion.\",\"authors\":\"Jian-Yun Zhou, Xin Zhang, Hai-Bin Gao, Ze Cao, Wei Sun\",\"doi\":\"10.5114/wiitm.2020.99350\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Subdural effusion is a common complication that occurs after decompressive craniectomy. According to the endoscopy results, the formation mechanism of subdural effusion after decompressive craniectomy was discussed.</p><p><strong>Aim: </strong>The morphological structure of subdural effusion in skull defects was observed with endoscopy, and endoscopic-assisted surgery was performed for subdural effusion.</p><p><strong>Material and methods: </strong>From January 2018 to March 2020, 19 cases of skull repair and treatment of subdural effusion were performed. The external wall of the capsule was kept intact during the operation, subdural effusion and surgical procedure of the subdural effusion under an endoscope could be observed, and the results of endoscopic observation were described and recorded. A hemostasis gauze was placed between the two layers of the subdural effusion cavity. Another 13 cases of skull defects with subdural effusion treated without endoscopy during the same time period were enrolled in the study as the control group. The postoperative disappearance of effusion and the incidence of postoperative complications were compared between the two groups.</p><p><strong>Results: </strong>Analysis with an endoscope revealed that all cases of subdural effusion in skull defects presented capsules. The main structures included the outer wall, boundary, inner wall, and fistula. The outer wall was made up of new tissue that had formed after removing the bone flap under the skin flap by artificial peeling under the condition of keeping the whole cavity. The inner wall consisted of thickened arachnoid, dura, and artificial dura. It presented with neovascularization networks, which showed a tendency to form new membrane structures through mutual adhesion and fusion. The inner and outer wall of the skull had fused to form the boundary of the cavity. Cerebrospinal fluid fistulas were detected in 31.6% of the internal walls. Subdural effusion was effectively treated in both the experimental group and the control group. Compared with the control group, complications in the experimental group were significantly reduced.</p><p><strong>Conclusions: </strong>The effusion cavity can be divided into three types based on its structural characteristics: fistula type, membrane type, and closed type. In this study, the formation mechanism of skull defects combined with subdural effusion was explored. This represents a new method for treating subdural effusion in which hemostasis gauze is placed between the two layers of the effusion cavity and cerebrospinal fluid fistula under an endoscope, which can effectively reduce the incidence of postoperative complications.</p>\",\"PeriodicalId\":520827,\"journal\":{\"name\":\"Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques\",\"volume\":\" \",\"pages\":\"219-226\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.5114/wiitm.2020.99350\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5114/wiitm.2020.99350\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/9/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5114/wiitm.2020.99350","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/9/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Endoscopic-assisted surgery for skull defects with subdural effusion.
Introduction: Subdural effusion is a common complication that occurs after decompressive craniectomy. According to the endoscopy results, the formation mechanism of subdural effusion after decompressive craniectomy was discussed.
Aim: The morphological structure of subdural effusion in skull defects was observed with endoscopy, and endoscopic-assisted surgery was performed for subdural effusion.
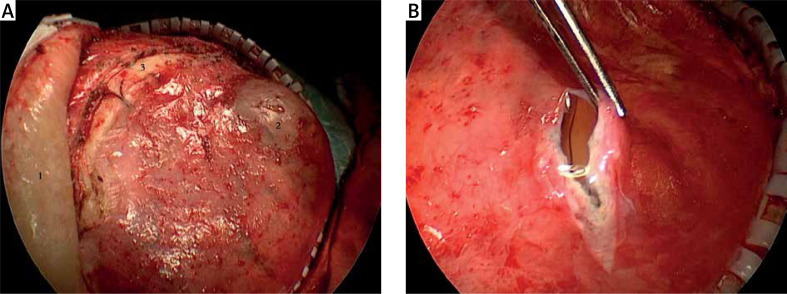
Material and methods: From January 2018 to March 2020, 19 cases of skull repair and treatment of subdural effusion were performed. The external wall of the capsule was kept intact during the operation, subdural effusion and surgical procedure of the subdural effusion under an endoscope could be observed, and the results of endoscopic observation were described and recorded. A hemostasis gauze was placed between the two layers of the subdural effusion cavity. Another 13 cases of skull defects with subdural effusion treated without endoscopy during the same time period were enrolled in the study as the control group. The postoperative disappearance of effusion and the incidence of postoperative complications were compared between the two groups.
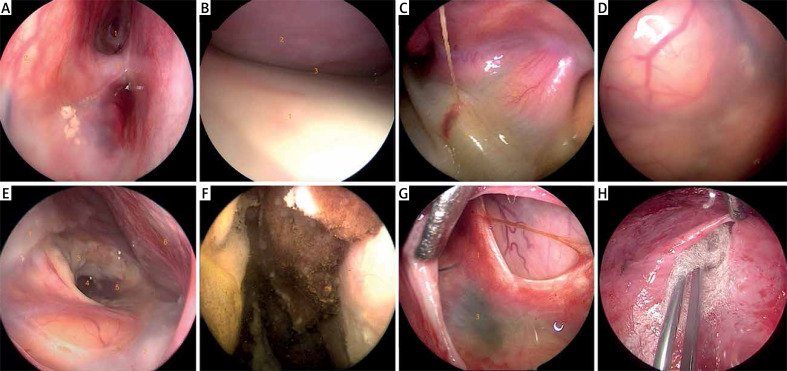
Results: Analysis with an endoscope revealed that all cases of subdural effusion in skull defects presented capsules. The main structures included the outer wall, boundary, inner wall, and fistula. The outer wall was made up of new tissue that had formed after removing the bone flap under the skin flap by artificial peeling under the condition of keeping the whole cavity. The inner wall consisted of thickened arachnoid, dura, and artificial dura. It presented with neovascularization networks, which showed a tendency to form new membrane structures through mutual adhesion and fusion. The inner and outer wall of the skull had fused to form the boundary of the cavity. Cerebrospinal fluid fistulas were detected in 31.6% of the internal walls. Subdural effusion was effectively treated in both the experimental group and the control group. Compared with the control group, complications in the experimental group were significantly reduced.
Conclusions: The effusion cavity can be divided into three types based on its structural characteristics: fistula type, membrane type, and closed type. In this study, the formation mechanism of skull defects combined with subdural effusion was explored. This represents a new method for treating subdural effusion in which hemostasis gauze is placed between the two layers of the effusion cavity and cerebrospinal fluid fistula under an endoscope, which can effectively reduce the incidence of postoperative complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


