Rune B Strandby, Rikard Ambrus, Linea L Ring, Nikolaj Nerup, Niels H Secher, Jens P Goetze, Michael P Achiam, Lars B Svendsen
{"title":"开放式食管切除术中TEA的早期激活会加重MTS相关的低血压。","authors":"Rune B Strandby, Rikard Ambrus, Linea L Ring, Nikolaj Nerup, Niels H Secher, Jens P Goetze, Michael P Achiam, Lars B Svendsen","doi":"10.2147/LRA.S294556","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>A mesenteric traction syndrome (MTS) is elicited by prostacyclin (PGI<sub>2</sub>)-induced vasodilation and identified by facial flushing, tachycardia, and hypotension during abdominal surgery. We evaluated whether thoracic epidural anesthesia (TEA) influences the incidence of MTS.</p><p><strong>Design: </strong>Randomized, blinded controlled trial.</p><p><strong>Setting: </strong>Single-center university hospital.</p><p><strong>Participants: </strong>Fifty patients undergoing open esophagectomy.</p><p><strong>Interventions: </strong>Patients were randomized to either early (EA, after induction of general anesthesia) or late activation of TEA (LA, after re-established gastric continuity). Plasma 6-keto-PGF<sub>1α</sub>, a stable metabolite of PGI<sub>2</sub> and interleukine-6 (IL6) were measured in plasma during surgery along with hemodynamic variables and MTS graded according to facial flushing together with plasma C-reactive protein on the third post-operative day.</p><p><strong>Results: </strong>Forty-five patients met the inclusion criteria. Development of MTS tended to be more prevalent with EA (n=13/25 [52%]) than with LA TEA (n=5/20 [25%], p=0.08). For patients who developed MTS, there was a transient increase in plasma 6-keto-PGF<sub>1α</sub> by 15 min of surgery and plasma IL6 (p<0.001) as C-reactive protein (P<0.009) increased. EA TEA influenced the amount of phenylephrine needed to maintain mean arterial pressure >60 mmHg in patients who developed MTS (0.16 [0.016-0.019] mg/min vs MTS and LA TEA 0.000 [0.000-0.005] mg/min, p<0.001).</p><p><strong>Conclusion: </strong>The incidence of MTS is not prevented by TEA in patients undergoing open esophagectomy. On the contrary, the risk of hypotension is increased in patients exposed to TEA during surgery, and the results suggest that it is advantageous to delay activation of TEA. Also, MTS seems to be associated with a systemic inflammatory response, maybe explaining the aggravated post-operative outcome.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"14 ","pages":"33-42"},"PeriodicalIF":1.9000,"publicationDate":"2021-03-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cc/4c/lra-14-33.PMC7936689.pdf","citationCount":"2","resultStr":"{\"title\":\"Hypotension Associated with MTS is Aggravated by Early Activation of TEA During Open Esophagectomy.\",\"authors\":\"Rune B Strandby, Rikard Ambrus, Linea L Ring, Nikolaj Nerup, Niels H Secher, Jens P Goetze, Michael P Achiam, Lars B Svendsen\",\"doi\":\"10.2147/LRA.S294556\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>A mesenteric traction syndrome (MTS) is elicited by prostacyclin (PGI<sub>2</sub>)-induced vasodilation and identified by facial flushing, tachycardia, and hypotension during abdominal surgery. We evaluated whether thoracic epidural anesthesia (TEA) influences the incidence of MTS.</p><p><strong>Design: </strong>Randomized, blinded controlled trial.</p><p><strong>Setting: </strong>Single-center university hospital.</p><p><strong>Participants: </strong>Fifty patients undergoing open esophagectomy.</p><p><strong>Interventions: </strong>Patients were randomized to either early (EA, after induction of general anesthesia) or late activation of TEA (LA, after re-established gastric continuity). Plasma 6-keto-PGF<sub>1α</sub>, a stable metabolite of PGI<sub>2</sub> and interleukine-6 (IL6) were measured in plasma during surgery along with hemodynamic variables and MTS graded according to facial flushing together with plasma C-reactive protein on the third post-operative day.</p><p><strong>Results: </strong>Forty-five patients met the inclusion criteria. Development of MTS tended to be more prevalent with EA (n=13/25 [52%]) than with LA TEA (n=5/20 [25%], p=0.08). For patients who developed MTS, there was a transient increase in plasma 6-keto-PGF<sub>1α</sub> by 15 min of surgery and plasma IL6 (p<0.001) as C-reactive protein (P<0.009) increased. EA TEA influenced the amount of phenylephrine needed to maintain mean arterial pressure >60 mmHg in patients who developed MTS (0.16 [0.016-0.019] mg/min vs MTS and LA TEA 0.000 [0.000-0.005] mg/min, p<0.001).</p><p><strong>Conclusion: </strong>The incidence of MTS is not prevented by TEA in patients undergoing open esophagectomy. On the contrary, the risk of hypotension is increased in patients exposed to TEA during surgery, and the results suggest that it is advantageous to delay activation of TEA. Also, MTS seems to be associated with a systemic inflammatory response, maybe explaining the aggravated post-operative outcome.</p>\",\"PeriodicalId\":18203,\"journal\":{\"name\":\"Local and Regional Anesthesia\",\"volume\":\"14 \",\"pages\":\"33-42\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2021-03-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cc/4c/lra-14-33.PMC7936689.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Local and Regional Anesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/LRA.S294556\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S294556","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Hypotension Associated with MTS is Aggravated by Early Activation of TEA During Open Esophagectomy.
Objective: A mesenteric traction syndrome (MTS) is elicited by prostacyclin (PGI2)-induced vasodilation and identified by facial flushing, tachycardia, and hypotension during abdominal surgery. We evaluated whether thoracic epidural anesthesia (TEA) influences the incidence of MTS.
Design: Randomized, blinded controlled trial.
Setting: Single-center university hospital.
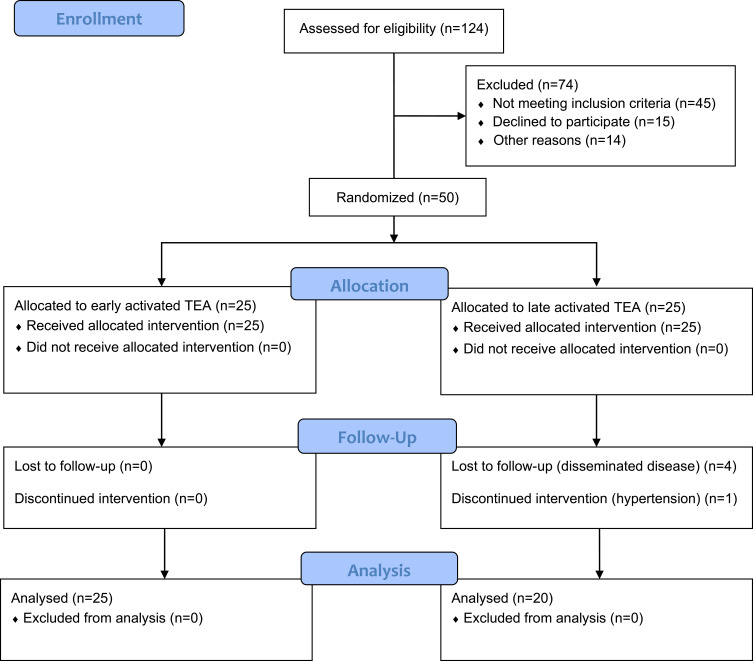
Participants: Fifty patients undergoing open esophagectomy.
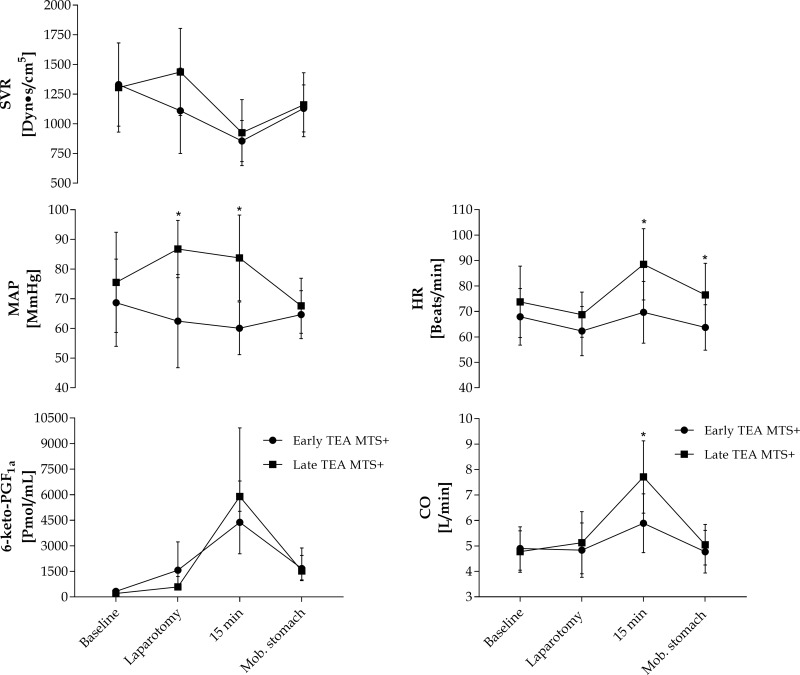
Interventions: Patients were randomized to either early (EA, after induction of general anesthesia) or late activation of TEA (LA, after re-established gastric continuity). Plasma 6-keto-PGF1α, a stable metabolite of PGI2 and interleukine-6 (IL6) were measured in plasma during surgery along with hemodynamic variables and MTS graded according to facial flushing together with plasma C-reactive protein on the third post-operative day.
Results: Forty-five patients met the inclusion criteria. Development of MTS tended to be more prevalent with EA (n=13/25 [52%]) than with LA TEA (n=5/20 [25%], p=0.08). For patients who developed MTS, there was a transient increase in plasma 6-keto-PGF1α by 15 min of surgery and plasma IL6 (p<0.001) as C-reactive protein (P<0.009) increased. EA TEA influenced the amount of phenylephrine needed to maintain mean arterial pressure >60 mmHg in patients who developed MTS (0.16 [0.016-0.019] mg/min vs MTS and LA TEA 0.000 [0.000-0.005] mg/min, p<0.001).
Conclusion: The incidence of MTS is not prevented by TEA in patients undergoing open esophagectomy. On the contrary, the risk of hypotension is increased in patients exposed to TEA during surgery, and the results suggest that it is advantageous to delay activation of TEA. Also, MTS seems to be associated with a systemic inflammatory response, maybe explaining the aggravated post-operative outcome.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


