Dodul Mondal, Sachin R Jhawar, Rihan Millevoi, Bruce G Haffty, Rahul R Parikh
{"title":"质子与光子屏气放射治疗左侧乳腺癌保乳术后:剂量学比较。","authors":"Dodul Mondal, Sachin R Jhawar, Rihan Millevoi, Bruce G Haffty, Rahul R Parikh","doi":"10.14338/IJPT-20-00026.1","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Radiation to breast, chest wall, and/or regional nodes is an integral component of breast cancer management in many situations. Irradiating left-sided breast and/or regional nodes may be technically challenging because of cardiac tolerance and subsequent risk of long-term cardiac complications. Deep inspiratory breath-hold (DIBH) technique physically separates cardiac structures away from radiation target volume, thus reducing cardiac dose with either photon (Ph) or proton beam therapy (PBT). The utility of combining PBT with DIBH is less well understood.</p><p><strong>Methods and materials: </strong>We compared photon-DIBH (Ph-DIBH) versus proton DIBH (Pr-DIBH) for different planning parameters, including target coverage and organ at risk (OAR) sparing. Necessary ethical permission was obtained from the institutional review board. Ten previous patients with irradiated, intact, left-sided breast and Ph-DIBH were replanned with PBT for dosimetric comparison. Clinically relevant normal OARs were contoured, and Ph plans were generated with parallel, opposed tangent beams and direct fields for supraclavicular and/or axillae whenever required. For proton planning, all targets were delineated individually and best possible coverage of planning target volume was achieved. Dose-volume histogram was analyzed to determine the difference in doses received by different OARs. Minimum and maximum dose (<i>D<sub>min</sub></i> and <i>D<sub>max</sub></i> ) as well as dose received by a specific volume of OAR were compared. Each patient's initial plan (Ph-DIBH) was used as a control for comparing newly devised PBT plan (Pr-DIBH). Matched, paired <i>t</i> tests were applied to determine any significant differences between the 2 plans.</p><p><strong>Results: </strong>Both the plans were adequate in target coverage. Dose to cardiac structure subunits and ipsilateral lung were significantly reduced with the proton breath-hold technique. Significant dose reduction with Pr-DIBH was observed in comparison to Ph-DIBH for mean dose (<i>D</i> <sub>mean</sub>) to the heart (0.23 Gy versus 1.19 Gy; <i>P</i> < .001); <i>D</i> <sub>mean</sub> to the left ventricle (0.25 Gy versus 1.7 Gy; <i>P</i> < .001); <i>D</i> <sub>mean</sub>, <i>D</i> <sub>max</sub>, and the half-maximal dose to the left anterior descending artery (1.15 Gy versus 5.54 Gy; <i>P</i> < .003; 7.7 Gy versus 22.15 Gy; <i>P</i> < .007; 1.61 Gy versus 4.42 Gy, <i>P</i> < .049); <i>D</i> <sub>max</sub> of the left circumflex coronary artery (0.13 Gy versus 1.35 Gy; <i>P</i> < .001) and <i>D</i> <sub>mean</sub>, the volume to the ipsilateral lung receiving 20 Gy and 5 Gy (2.28 Gy versus 8.04 Gy; <i>P</i> < .001; 2.36 Gy versus 15.54 Gy, <i>P</i> < .001; 13.9 Gy versus 30.28 Gy; <i>P</i> = .002). However, skin dose and contralateral breast dose were not significantly improved with proton.</p><p><strong>Conclusion: </strong>This comparative dosimetric study showed significant benefit of Pr-DIBH technique compared with Ph-DIBH in terms of cardiopulmonary sparing and may be the area of future clinical research.</p>","PeriodicalId":36923,"journal":{"name":"International Journal of Particle Therapy","volume":"7 3","pages":"24-33"},"PeriodicalIF":2.1000,"publicationDate":"2020-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7886268/pdf/","citationCount":"7","resultStr":"{\"title\":\"Proton versus Photon Breath-Hold Radiation for Left-Sided Breast Cancer after Breast-Conserving Surgery: A Dosimetric Comparison.\",\"authors\":\"Dodul Mondal, Sachin R Jhawar, Rihan Millevoi, Bruce G Haffty, Rahul R Parikh\",\"doi\":\"10.14338/IJPT-20-00026.1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Radiation to breast, chest wall, and/or regional nodes is an integral component of breast cancer management in many situations. Irradiating left-sided breast and/or regional nodes may be technically challenging because of cardiac tolerance and subsequent risk of long-term cardiac complications. Deep inspiratory breath-hold (DIBH) technique physically separates cardiac structures away from radiation target volume, thus reducing cardiac dose with either photon (Ph) or proton beam therapy (PBT). The utility of combining PBT with DIBH is less well understood.</p><p><strong>Methods and materials: </strong>We compared photon-DIBH (Ph-DIBH) versus proton DIBH (Pr-DIBH) for different planning parameters, including target coverage and organ at risk (OAR) sparing. Necessary ethical permission was obtained from the institutional review board. Ten previous patients with irradiated, intact, left-sided breast and Ph-DIBH were replanned with PBT for dosimetric comparison. Clinically relevant normal OARs were contoured, and Ph plans were generated with parallel, opposed tangent beams and direct fields for supraclavicular and/or axillae whenever required. For proton planning, all targets were delineated individually and best possible coverage of planning target volume was achieved. Dose-volume histogram was analyzed to determine the difference in doses received by different OARs. Minimum and maximum dose (<i>D<sub>min</sub></i> and <i>D<sub>max</sub></i> ) as well as dose received by a specific volume of OAR were compared. Each patient's initial plan (Ph-DIBH) was used as a control for comparing newly devised PBT plan (Pr-DIBH). Matched, paired <i>t</i> tests were applied to determine any significant differences between the 2 plans.</p><p><strong>Results: </strong>Both the plans were adequate in target coverage. Dose to cardiac structure subunits and ipsilateral lung were significantly reduced with the proton breath-hold technique. Significant dose reduction with Pr-DIBH was observed in comparison to Ph-DIBH for mean dose (<i>D</i> <sub>mean</sub>) to the heart (0.23 Gy versus 1.19 Gy; <i>P</i> < .001); <i>D</i> <sub>mean</sub> to the left ventricle (0.25 Gy versus 1.7 Gy; <i>P</i> < .001); <i>D</i> <sub>mean</sub>, <i>D</i> <sub>max</sub>, and the half-maximal dose to the left anterior descending artery (1.15 Gy versus 5.54 Gy; <i>P</i> < .003; 7.7 Gy versus 22.15 Gy; <i>P</i> < .007; 1.61 Gy versus 4.42 Gy, <i>P</i> < .049); <i>D</i> <sub>max</sub> of the left circumflex coronary artery (0.13 Gy versus 1.35 Gy; <i>P</i> < .001) and <i>D</i> <sub>mean</sub>, the volume to the ipsilateral lung receiving 20 Gy and 5 Gy (2.28 Gy versus 8.04 Gy; <i>P</i> < .001; 2.36 Gy versus 15.54 Gy, <i>P</i> < .001; 13.9 Gy versus 30.28 Gy; <i>P</i> = .002). However, skin dose and contralateral breast dose were not significantly improved with proton.</p><p><strong>Conclusion: </strong>This comparative dosimetric study showed significant benefit of Pr-DIBH technique compared with Ph-DIBH in terms of cardiopulmonary sparing and may be the area of future clinical research.</p>\",\"PeriodicalId\":36923,\"journal\":{\"name\":\"International Journal of Particle Therapy\",\"volume\":\"7 3\",\"pages\":\"24-33\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2020-12-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7886268/pdf/\",\"citationCount\":\"7\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Particle Therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14338/IJPT-20-00026.1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Particle Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14338/IJPT-20-00026.1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 7
摘要
目的:在许多情况下,乳房、胸壁和/或局部淋巴结放射治疗是乳腺癌治疗的一个组成部分。由于心脏耐受性和随后的长期心脏并发症风险,照射左侧乳房和/或局部淋巴结在技术上可能具有挑战性。深吸气式憋气(DIBH)技术将心脏结构从辐射靶体积中分离出来,从而降低了光子(Ph)或质子束治疗(PBT)的心脏剂量。PBT联合DIBH的效用还不太清楚。方法和材料:我们比较了光子DIBH (Ph-DIBH)和质子DIBH (Pr-DIBH)在不同的规划参数下,包括靶覆盖和危险器官(OAR)保留。从机构审查委员会获得了必要的伦理许可。10例既往的完整左侧乳房和Ph-DIBH患者重新计划PBT进行剂量学比较。对临床相关的正常桨进行轮廓,并根据需要对锁骨上和/或腋窝进行平行、相对切线束和直接场生成Ph图。对于质子规划,所有目标都被单独描绘,并实现了规划目标体积的最佳覆盖。分析剂量-体积直方图,以确定不同桨接受剂量的差异。比较了最小和最大剂量(Dmin和Dmax)以及特定体积OAR所接受的剂量。以每位患者的初始方案(Ph-DIBH)作为对照,比较新设计的PBT方案(Pr-DIBH)。采用配对t检验来确定两个方案之间是否存在显著差异。结果:两种方案的目标覆盖率均较好。质子屏气技术对心脏结构亚单位和同侧肺的剂量显著降低。与Ph-DIBH相比,Pr-DIBH对心脏的平均剂量(D平均值)显著降低(0.23 Gy对1.19 Gy;左心室P - D平均值(0.25 Gy vs 1.7 Gy;左前降支的ppd均值、dmax和半最大剂量(1.15 Gy vs 5.54 Gy;左旋冠状动脉P P P D max (0.13 Gy vs 1.35 Gy;P - D平均,同侧肺容积分别为20 Gy和5 Gy (2.28 Gy vs 8.04 Gy;p p p = .002)。然而,皮肤剂量和对侧乳房剂量在质子治疗后没有明显改善。结论:本比较剂量学研究显示Pr-DIBH技术与Ph-DIBH技术相比在心肺保护方面有显著的优势,可能是未来临床研究的领域。
Proton versus Photon Breath-Hold Radiation for Left-Sided Breast Cancer after Breast-Conserving Surgery: A Dosimetric Comparison.
Purpose: Radiation to breast, chest wall, and/or regional nodes is an integral component of breast cancer management in many situations. Irradiating left-sided breast and/or regional nodes may be technically challenging because of cardiac tolerance and subsequent risk of long-term cardiac complications. Deep inspiratory breath-hold (DIBH) technique physically separates cardiac structures away from radiation target volume, thus reducing cardiac dose with either photon (Ph) or proton beam therapy (PBT). The utility of combining PBT with DIBH is less well understood.
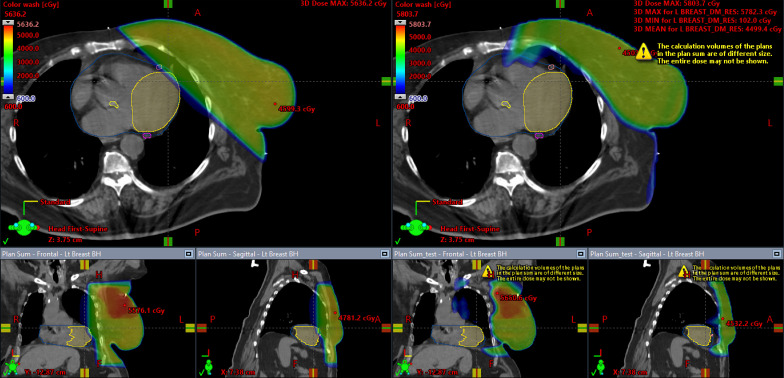
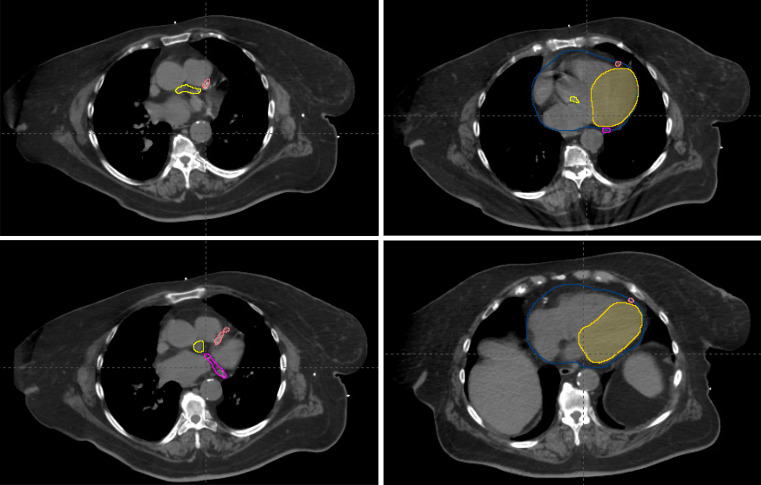
Methods and materials: We compared photon-DIBH (Ph-DIBH) versus proton DIBH (Pr-DIBH) for different planning parameters, including target coverage and organ at risk (OAR) sparing. Necessary ethical permission was obtained from the institutional review board. Ten previous patients with irradiated, intact, left-sided breast and Ph-DIBH were replanned with PBT for dosimetric comparison. Clinically relevant normal OARs were contoured, and Ph plans were generated with parallel, opposed tangent beams and direct fields for supraclavicular and/or axillae whenever required. For proton planning, all targets were delineated individually and best possible coverage of planning target volume was achieved. Dose-volume histogram was analyzed to determine the difference in doses received by different OARs. Minimum and maximum dose (Dmin and Dmax ) as well as dose received by a specific volume of OAR were compared. Each patient's initial plan (Ph-DIBH) was used as a control for comparing newly devised PBT plan (Pr-DIBH). Matched, paired t tests were applied to determine any significant differences between the 2 plans.
Results: Both the plans were adequate in target coverage. Dose to cardiac structure subunits and ipsilateral lung were significantly reduced with the proton breath-hold technique. Significant dose reduction with Pr-DIBH was observed in comparison to Ph-DIBH for mean dose (Dmean) to the heart (0.23 Gy versus 1.19 Gy; P < .001); Dmean to the left ventricle (0.25 Gy versus 1.7 Gy; P < .001); Dmean, Dmax, and the half-maximal dose to the left anterior descending artery (1.15 Gy versus 5.54 Gy; P < .003; 7.7 Gy versus 22.15 Gy; P < .007; 1.61 Gy versus 4.42 Gy, P < .049); Dmax of the left circumflex coronary artery (0.13 Gy versus 1.35 Gy; P < .001) and Dmean, the volume to the ipsilateral lung receiving 20 Gy and 5 Gy (2.28 Gy versus 8.04 Gy; P < .001; 2.36 Gy versus 15.54 Gy, P < .001; 13.9 Gy versus 30.28 Gy; P = .002). However, skin dose and contralateral breast dose were not significantly improved with proton.
Conclusion: This comparative dosimetric study showed significant benefit of Pr-DIBH technique compared with Ph-DIBH in terms of cardiopulmonary sparing and may be the area of future clinical research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


