{"title":"我不是一个诊断:青少年对用户参与和共同决策在精神卫生保健的观点。","authors":"Stig Bjønness, Trond Grønnestad, Marianne Storm","doi":"10.21307/sjcapp-2020-014","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adolescents have the right to be involved in decisions affecting their healthcare. More knowledge is needed to provide quality healthcare services that is both suitable for adolescents and in line with policy. Shared decision-making has the potential to combine user participation and evidence-based treatment. Research and governmental policies emphasize shared decision-making as key for high quality mental healthcare services.</p><p><strong>Objective: </strong>To explore adolescents' experiences with user participation and shared decision-making in mental healthcare inpatient units.</p><p><strong>Method: </strong>We carried out ten in-depth interviews with adolescents (16-18 years old) in this qualitative study. The participants were admitted to four mental healthcare inpatient clinics in Norway. Transcribed interviews were subjected to qualitative content analysis.</p><p><strong>Results: </strong>Five themes were identified, representing the adolescents' view of gaining trust, getting help, being understood, being diagnosed and labeled, being pushed, and making a customized treatment plan. Psychoeducational information, mutual trust, and a therapeutic relationship between patients and therapists were considered prerequisites for shared decision-making. For adolescents to be labeled with a diagnosis or forced into a treatment regimen that they did not initiate or control tended to elicit strong resistance. User involvement at admission, participation in the treatment plan, individualized treatment, and collaboration among healthcare professionals were emphasized.</p><p><strong>Conclusions: </strong>Routines for participation and involvement of adolescents prior to inpatient admission is recommended. Shared decision-making has the potential to increase adolescents' engagement and reduce the incidence of involuntary treatment and re-admission to inpatient clinics. In this study, shared decision-making is linked to empowerment and less to standardized decision tools. To be labeled and dominated by healthcare professionals can be a barrier to adolescents' participation in treatment. We suggest placing less emphasis on diagnoses and more on individualized treatment.</p>","PeriodicalId":42655,"journal":{"name":"Scandinavian Journal of Child and Adolescent Psychiatry and Psychology","volume":"8 ","pages":"139-148"},"PeriodicalIF":1.0000,"publicationDate":"2020-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6c/28/sjcapp-08-014.PMC7863730.pdf","citationCount":"12","resultStr":"{\"title\":\"I'm not a diagnosis: Adolescents' perspectives on user participation and shared decision-making in mental healthcare.\",\"authors\":\"Stig Bjønness, Trond Grønnestad, Marianne Storm\",\"doi\":\"10.21307/sjcapp-2020-014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Adolescents have the right to be involved in decisions affecting their healthcare. More knowledge is needed to provide quality healthcare services that is both suitable for adolescents and in line with policy. Shared decision-making has the potential to combine user participation and evidence-based treatment. Research and governmental policies emphasize shared decision-making as key for high quality mental healthcare services.</p><p><strong>Objective: </strong>To explore adolescents' experiences with user participation and shared decision-making in mental healthcare inpatient units.</p><p><strong>Method: </strong>We carried out ten in-depth interviews with adolescents (16-18 years old) in this qualitative study. The participants were admitted to four mental healthcare inpatient clinics in Norway. Transcribed interviews were subjected to qualitative content analysis.</p><p><strong>Results: </strong>Five themes were identified, representing the adolescents' view of gaining trust, getting help, being understood, being diagnosed and labeled, being pushed, and making a customized treatment plan. Psychoeducational information, mutual trust, and a therapeutic relationship between patients and therapists were considered prerequisites for shared decision-making. For adolescents to be labeled with a diagnosis or forced into a treatment regimen that they did not initiate or control tended to elicit strong resistance. User involvement at admission, participation in the treatment plan, individualized treatment, and collaboration among healthcare professionals were emphasized.</p><p><strong>Conclusions: </strong>Routines for participation and involvement of adolescents prior to inpatient admission is recommended. Shared decision-making has the potential to increase adolescents' engagement and reduce the incidence of involuntary treatment and re-admission to inpatient clinics. In this study, shared decision-making is linked to empowerment and less to standardized decision tools. To be labeled and dominated by healthcare professionals can be a barrier to adolescents' participation in treatment. We suggest placing less emphasis on diagnoses and more on individualized treatment.</p>\",\"PeriodicalId\":42655,\"journal\":{\"name\":\"Scandinavian Journal of Child and Adolescent Psychiatry and Psychology\",\"volume\":\"8 \",\"pages\":\"139-148\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2020-09-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6c/28/sjcapp-08-014.PMC7863730.pdf\",\"citationCount\":\"12\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scandinavian Journal of Child and Adolescent Psychiatry and Psychology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21307/sjcapp-2020-014\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PSYCHIATRY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Child and Adolescent Psychiatry and Psychology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21307/sjcapp-2020-014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PSYCHIATRY","Score":null,"Total":0}
I'm not a diagnosis: Adolescents' perspectives on user participation and shared decision-making in mental healthcare.
Background: Adolescents have the right to be involved in decisions affecting their healthcare. More knowledge is needed to provide quality healthcare services that is both suitable for adolescents and in line with policy. Shared decision-making has the potential to combine user participation and evidence-based treatment. Research and governmental policies emphasize shared decision-making as key for high quality mental healthcare services.
Objective: To explore adolescents' experiences with user participation and shared decision-making in mental healthcare inpatient units.
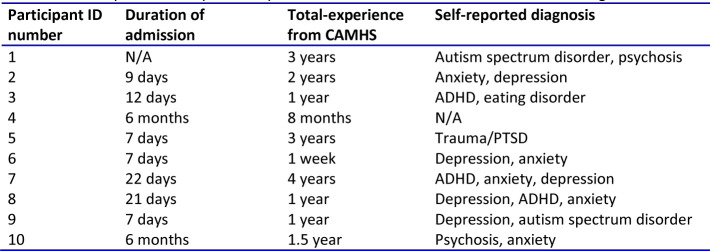
Method: We carried out ten in-depth interviews with adolescents (16-18 years old) in this qualitative study. The participants were admitted to four mental healthcare inpatient clinics in Norway. Transcribed interviews were subjected to qualitative content analysis.
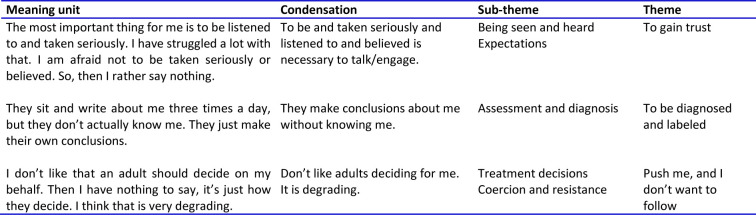
Results: Five themes were identified, representing the adolescents' view of gaining trust, getting help, being understood, being diagnosed and labeled, being pushed, and making a customized treatment plan. Psychoeducational information, mutual trust, and a therapeutic relationship between patients and therapists were considered prerequisites for shared decision-making. For adolescents to be labeled with a diagnosis or forced into a treatment regimen that they did not initiate or control tended to elicit strong resistance. User involvement at admission, participation in the treatment plan, individualized treatment, and collaboration among healthcare professionals were emphasized.
Conclusions: Routines for participation and involvement of adolescents prior to inpatient admission is recommended. Shared decision-making has the potential to increase adolescents' engagement and reduce the incidence of involuntary treatment and re-admission to inpatient clinics. In this study, shared decision-making is linked to empowerment and less to standardized decision tools. To be labeled and dominated by healthcare professionals can be a barrier to adolescents' participation in treatment. We suggest placing less emphasis on diagnoses and more on individualized treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


