{"title":"冠状动脉疾病终生维持阶段的身体活动障碍和患者特征分析:一项区域混合方法的试点研究","authors":"Morgane Molina, Fabienne Durand, Henri Meric","doi":"10.3389/fresc.2025.1659925","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Despite proven benefits, adherence to physical activity (PA) during the lifelong maintenance phase of cardiac rehabilitation (CR) remains suboptimal. Understanding territorial-specific barriers is essential for developing targeted interventions. This pilot study aimed to (1) identify principal barriers to PA among coronary artery disease (CAD) patients in lifelong maintenance Phase CR in a specific territory of southern France, and (2) characterize distinct patient profiles using unsupervised machine learning.</p><p><strong>Methods: </strong>Socio-demographic data, completion of a full Phase II CR and behavioral characteristics related to PA during the lifelong maintenance Phase were collected with a LimeSurvey questionnaire. A modified Delphi method was employed with CAD patients (<i>n</i> = 26, subsequently, <i>n</i> = 13 in round 2) who had completed a supervised Phase II CR. Barriers were categorized and ranked using Likert scales. K-means clustering analysis was then applied to identify homogeneous patient subgroups based on barrier patterns.</p><p><strong>Results: </strong>Nine barrier categories emerged, with environment (8.3 ± 1.0), motivation (7.7 ± 1.4), and exercise tolerance (6.3 ± 1.2) ranking highest. Kendall's W = 0.64 (<i>p</i> < 0.001) indicated a significant consensus. Three cluster were identified: Cluster 1 (38.46%) characterized by physical deconditioning; Cluster 2 (23.07%) by environmental and motivational constraints; Cluster 3 (38.46%) by organizational limitations. Significant between-cluster differences were observed for: environmental barriers (H = 7.82, <i>p</i> = 0.02), motivation (H = 8.14, <i>p</i> = 0.017), and professional obligations (H = 6.93, <i>p</i> = 0.031).</p><p><strong>Conclusion: </strong>This mixed-methods approach revealed complex, interrelated barriers to PA maintenance. The identification of distinct CAD patient profiles suggests that personalized intervention strategies, rather than one-size-fits-all approaches, may enhance long-term adherence to PA in lifelong maintenance Phase CR.</p>","PeriodicalId":73102,"journal":{"name":"Frontiers in rehabilitation sciences","volume":"6 ","pages":"1659925"},"PeriodicalIF":1.9000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12521154/pdf/","citationCount":"0","resultStr":"{\"title\":\"Barriers to physical activity and patient profiling in the lifelong maintenance phase of coronary artery disease: a territorial mixed-methods pilot study.\",\"authors\":\"Morgane Molina, Fabienne Durand, Henri Meric\",\"doi\":\"10.3389/fresc.2025.1659925\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Despite proven benefits, adherence to physical activity (PA) during the lifelong maintenance phase of cardiac rehabilitation (CR) remains suboptimal. Understanding territorial-specific barriers is essential for developing targeted interventions. This pilot study aimed to (1) identify principal barriers to PA among coronary artery disease (CAD) patients in lifelong maintenance Phase CR in a specific territory of southern France, and (2) characterize distinct patient profiles using unsupervised machine learning.</p><p><strong>Methods: </strong>Socio-demographic data, completion of a full Phase II CR and behavioral characteristics related to PA during the lifelong maintenance Phase were collected with a LimeSurvey questionnaire. A modified Delphi method was employed with CAD patients (<i>n</i> = 26, subsequently, <i>n</i> = 13 in round 2) who had completed a supervised Phase II CR. Barriers were categorized and ranked using Likert scales. K-means clustering analysis was then applied to identify homogeneous patient subgroups based on barrier patterns.</p><p><strong>Results: </strong>Nine barrier categories emerged, with environment (8.3 ± 1.0), motivation (7.7 ± 1.4), and exercise tolerance (6.3 ± 1.2) ranking highest. Kendall's W = 0.64 (<i>p</i> < 0.001) indicated a significant consensus. Three cluster were identified: Cluster 1 (38.46%) characterized by physical deconditioning; Cluster 2 (23.07%) by environmental and motivational constraints; Cluster 3 (38.46%) by organizational limitations. Significant between-cluster differences were observed for: environmental barriers (H = 7.82, <i>p</i> = 0.02), motivation (H = 8.14, <i>p</i> = 0.017), and professional obligations (H = 6.93, <i>p</i> = 0.031).</p><p><strong>Conclusion: </strong>This mixed-methods approach revealed complex, interrelated barriers to PA maintenance. The identification of distinct CAD patient profiles suggests that personalized intervention strategies, rather than one-size-fits-all approaches, may enhance long-term adherence to PA in lifelong maintenance Phase CR.</p>\",\"PeriodicalId\":73102,\"journal\":{\"name\":\"Frontiers in rehabilitation sciences\",\"volume\":\"6 \",\"pages\":\"1659925\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12521154/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in rehabilitation sciences\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/fresc.2025.1659925\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"REHABILITATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in rehabilitation sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fresc.2025.1659925","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 0
摘要
导读:尽管已证实有益处,但在心脏康复(CR)的终身维持阶段坚持体育活动(PA)仍然不是最佳选择。了解特定地区的障碍对于制定有针对性的干预措施至关重要。该试点研究旨在(1)在法国南部的特定地区,确定冠状动脉疾病(CAD)患者终身维持期CR的主要障碍,以及(2)使用无监督机器学习表征不同的患者概况。方法:通过limessurvey问卷收集社会人口学数据、完整的II期CR完成情况以及终身维持阶段与PA相关的行为特征。对完成监督II期CR的CAD患者(n = 26,随后在第2轮中n = 13)采用改进的德尔菲法。使用李克特量表对障碍进行分类和排名。然后应用k -均值聚类分析来确定基于屏障模式的同质患者亚组。结果:共出现9个障碍类别,其中环境障碍(8.3±1.0)、动机障碍(7.7±1.4)、运动耐量障碍(6.3±1.2)最高。肯德尔的W = 0.64 (p p = 0.02),动机(H = 8.14, p = 0.017),和职业义务(H = 6.93, p = 0.031)。结论:这种混合方法揭示了PA维持的复杂、相互关联的障碍。识别不同的CAD患者特征表明,个性化的干预策略,而不是一刀切的方法,可能会提高终身维持CR期患者对PA的长期依从性。
Barriers to physical activity and patient profiling in the lifelong maintenance phase of coronary artery disease: a territorial mixed-methods pilot study.
Introduction: Despite proven benefits, adherence to physical activity (PA) during the lifelong maintenance phase of cardiac rehabilitation (CR) remains suboptimal. Understanding territorial-specific barriers is essential for developing targeted interventions. This pilot study aimed to (1) identify principal barriers to PA among coronary artery disease (CAD) patients in lifelong maintenance Phase CR in a specific territory of southern France, and (2) characterize distinct patient profiles using unsupervised machine learning.
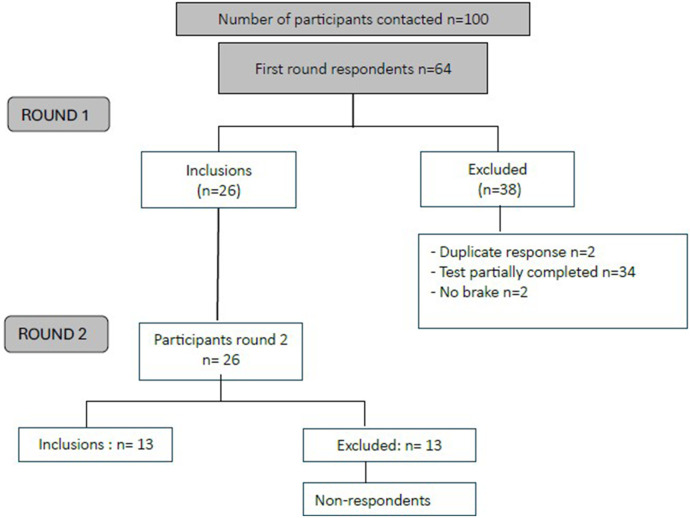
Methods: Socio-demographic data, completion of a full Phase II CR and behavioral characteristics related to PA during the lifelong maintenance Phase were collected with a LimeSurvey questionnaire. A modified Delphi method was employed with CAD patients (n = 26, subsequently, n = 13 in round 2) who had completed a supervised Phase II CR. Barriers were categorized and ranked using Likert scales. K-means clustering analysis was then applied to identify homogeneous patient subgroups based on barrier patterns.
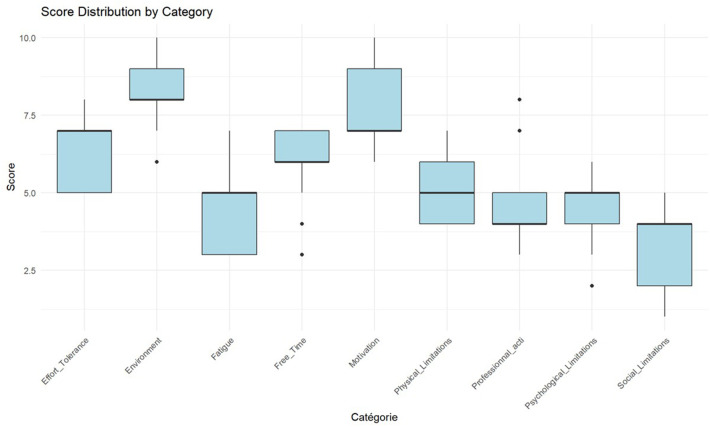
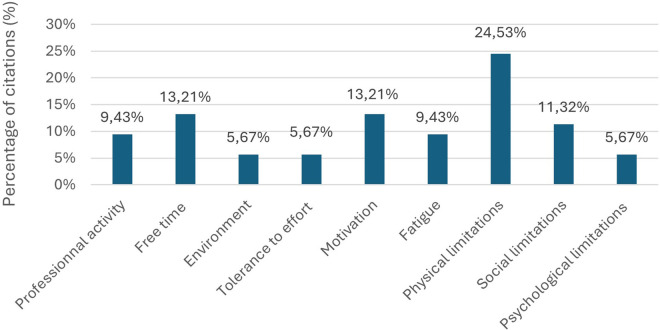
Results: Nine barrier categories emerged, with environment (8.3 ± 1.0), motivation (7.7 ± 1.4), and exercise tolerance (6.3 ± 1.2) ranking highest. Kendall's W = 0.64 (p < 0.001) indicated a significant consensus. Three cluster were identified: Cluster 1 (38.46%) characterized by physical deconditioning; Cluster 2 (23.07%) by environmental and motivational constraints; Cluster 3 (38.46%) by organizational limitations. Significant between-cluster differences were observed for: environmental barriers (H = 7.82, p = 0.02), motivation (H = 8.14, p = 0.017), and professional obligations (H = 6.93, p = 0.031).
Conclusion: This mixed-methods approach revealed complex, interrelated barriers to PA maintenance. The identification of distinct CAD patient profiles suggests that personalized intervention strategies, rather than one-size-fits-all approaches, may enhance long-term adherence to PA in lifelong maintenance Phase CR.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


