{"title":"重症急性胰腺炎患者早期预防性抗凝和住院死亡率:一项回顾性队列研究","authors":"Haodong Zhao, Hui Liu, Jiongjiong Cheng, Jia Chen, Shuo Li, Yaowei Sun, Yu Wang","doi":"10.2147/OAEM.S539104","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To investigate the association between early prophylactic anticoagulation and in-hospital mortality in ICU patients with severe acute pancreatitis.</p><p><strong>Patients and methods: </strong>This retrospective cohort study used data from the MIMIC-IV database (v3.1), including adult ICU patients diagnosed with SAP between 2008 and 2019. Patients receiving therapeutic anticoagulation were excluded. Early prophylactic anticoagulation was defined as subcutaneous heparin or enoxaparin administered within 24 hours of ICU admission. The primary outcome was in-hospital mortality. Multivariable Cox regression models with multiple imputation and propensity score matching were used to adjust for confounding.</p><p><strong>Results: </strong>Among 1341 eligible patients, 286 (21.3%) received early prophylactic anticoagulation. While crude in-hospital mortality was not significantly different between groups, patients receiving early anticoagulation had significantly lower in-hospital mortality (Log-rank P = 0.015). Multivariable Cox models confirmed a consistent protective association across imputed datasets (HRs ranging from 0.60 to 0.62; all P < 0.05). Subgroup analysis showed no significant interaction across age, gender, or comorbidity status. After 1:1 propensity score matching (n = 284 pairs), the mortality benefit persisted (HR = 0.51; 95% CI: 0.32-0.82; P = 0.005). Additional sensitivity analyses yielded similar results.</p><p><strong>Conclusion: </strong>Early prophylactic anticoagulation within 24 hours of ICU admission was associated with reduced in-hospital mortality in patients with severe acute pancreatitis. These findings suggest potential benefits of early anticoagulation in this high-risk population and warrant further prospective validation.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"17 ","pages":"289-300"},"PeriodicalIF":1.5000,"publicationDate":"2025-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12506791/pdf/","citationCount":"0","resultStr":"{\"title\":\"Early Prophylactic Anticoagulation and In-Hospital Mortality in Patients with Severe Acute Pancreatitis: A Retrospective Cohort Study.\",\"authors\":\"Haodong Zhao, Hui Liu, Jiongjiong Cheng, Jia Chen, Shuo Li, Yaowei Sun, Yu Wang\",\"doi\":\"10.2147/OAEM.S539104\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To investigate the association between early prophylactic anticoagulation and in-hospital mortality in ICU patients with severe acute pancreatitis.</p><p><strong>Patients and methods: </strong>This retrospective cohort study used data from the MIMIC-IV database (v3.1), including adult ICU patients diagnosed with SAP between 2008 and 2019. Patients receiving therapeutic anticoagulation were excluded. Early prophylactic anticoagulation was defined as subcutaneous heparin or enoxaparin administered within 24 hours of ICU admission. The primary outcome was in-hospital mortality. Multivariable Cox regression models with multiple imputation and propensity score matching were used to adjust for confounding.</p><p><strong>Results: </strong>Among 1341 eligible patients, 286 (21.3%) received early prophylactic anticoagulation. While crude in-hospital mortality was not significantly different between groups, patients receiving early anticoagulation had significantly lower in-hospital mortality (Log-rank P = 0.015). Multivariable Cox models confirmed a consistent protective association across imputed datasets (HRs ranging from 0.60 to 0.62; all P < 0.05). Subgroup analysis showed no significant interaction across age, gender, or comorbidity status. After 1:1 propensity score matching (n = 284 pairs), the mortality benefit persisted (HR = 0.51; 95% CI: 0.32-0.82; P = 0.005). Additional sensitivity analyses yielded similar results.</p><p><strong>Conclusion: </strong>Early prophylactic anticoagulation within 24 hours of ICU admission was associated with reduced in-hospital mortality in patients with severe acute pancreatitis. These findings suggest potential benefits of early anticoagulation in this high-risk population and warrant further prospective validation.</p>\",\"PeriodicalId\":45096,\"journal\":{\"name\":\"Open Access Emergency Medicine\",\"volume\":\"17 \",\"pages\":\"289-300\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-10-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12506791/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S539104\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S539104","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
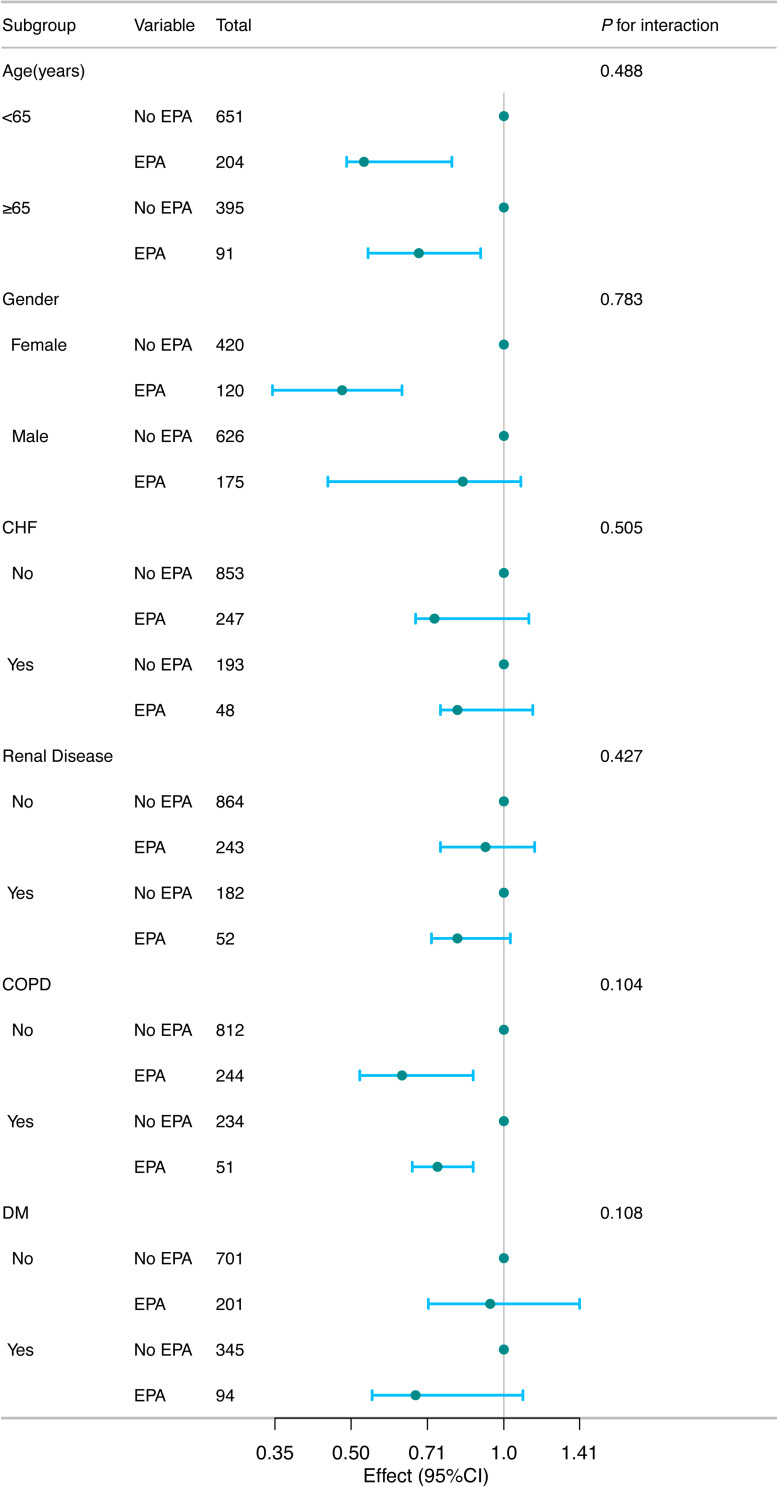
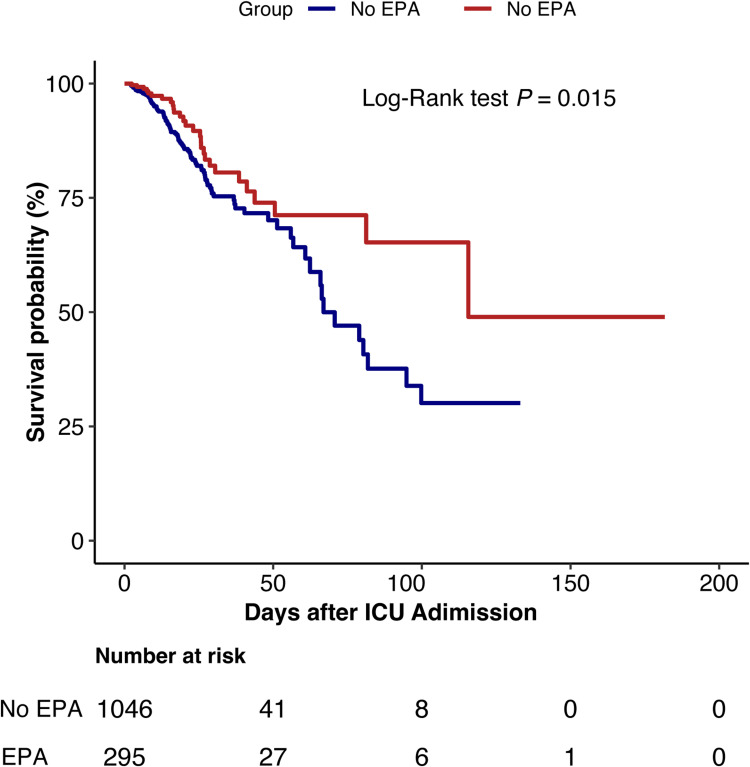
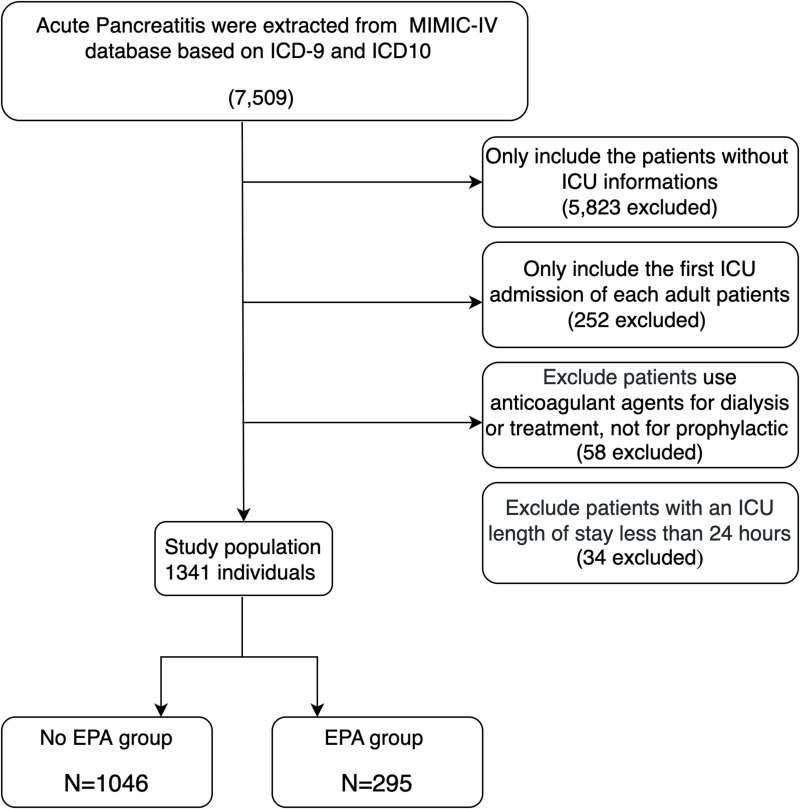
目的:探讨重症急性胰腺炎ICU患者早期预防性抗凝治疗与住院死亡率的关系。患者和方法:这项回顾性队列研究使用了MIMIC-IV数据库(v3.1)的数据,包括2008年至2019年间诊断为SAP的成年ICU患者。排除接受治疗性抗凝治疗的患者。早期预防性抗凝定义为在ICU入院24小时内皮下给予肝素或依诺肝素。主要终点是住院死亡率。采用多变量Cox回归模型进行多重输入和倾向评分匹配,以调整混杂因素。结果:1341例符合条件的患者中,286例(21.3%)接受了早期预防性抗凝治疗。虽然两组之间的住院死亡率无显著差异,但早期抗凝治疗患者的住院死亡率显著降低(Log-rank P = 0.015)。多变量Cox模型证实了输入数据集之间一致的保护性关联(hr范围为0.60至0.62,均P < 0.05)。亚组分析显示,年龄、性别或合并症状态之间没有显著的相互作用。经1:1倾向评分匹配(n = 284对)后,死亡率获益持续存在(HR = 0.51; 95% CI: 0.32-0.82; P = 0.005)。另外的敏感性分析也得出了类似的结果。结论:重症急性胰腺炎患者入院24小时内早期预防性抗凝可降低住院死亡率。这些发现提示在高危人群中早期抗凝治疗的潜在益处,需要进一步的前瞻性验证。
Early Prophylactic Anticoagulation and In-Hospital Mortality in Patients with Severe Acute Pancreatitis: A Retrospective Cohort Study.
Purpose: To investigate the association between early prophylactic anticoagulation and in-hospital mortality in ICU patients with severe acute pancreatitis.
Patients and methods: This retrospective cohort study used data from the MIMIC-IV database (v3.1), including adult ICU patients diagnosed with SAP between 2008 and 2019. Patients receiving therapeutic anticoagulation were excluded. Early prophylactic anticoagulation was defined as subcutaneous heparin or enoxaparin administered within 24 hours of ICU admission. The primary outcome was in-hospital mortality. Multivariable Cox regression models with multiple imputation and propensity score matching were used to adjust for confounding.
Results: Among 1341 eligible patients, 286 (21.3%) received early prophylactic anticoagulation. While crude in-hospital mortality was not significantly different between groups, patients receiving early anticoagulation had significantly lower in-hospital mortality (Log-rank P = 0.015). Multivariable Cox models confirmed a consistent protective association across imputed datasets (HRs ranging from 0.60 to 0.62; all P < 0.05). Subgroup analysis showed no significant interaction across age, gender, or comorbidity status. After 1:1 propensity score matching (n = 284 pairs), the mortality benefit persisted (HR = 0.51; 95% CI: 0.32-0.82; P = 0.005). Additional sensitivity analyses yielded similar results.
Conclusion: Early prophylactic anticoagulation within 24 hours of ICU admission was associated with reduced in-hospital mortality in patients with severe acute pancreatitis. These findings suggest potential benefits of early anticoagulation in this high-risk population and warrant further prospective validation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


