{"title":"肾移植术后12年富浆细胞急性排斥引起慢性活动性t细胞介导的排斥1例。","authors":"Ayaka Hayashi, Izumi Yamamoto, Mayuko Kawabe, Yutaro Ohki, Akimitsu Kobayashi, Fumihiko Urabe, Takafumi Yanagisawa, Shunsuke Tsuzuki, Jun Miki, Takahiro Kimura, Ichiro Ohkido, Nobuo Tsuboi, Hiroyasu Yamamoto, Takashi Yokoo","doi":"10.1159/000547828","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Plasma cell rich-acute rejection (PCAR) is a variant of T-cell-mediated rejection in kidney transplantation. Its pathogenesis remains unknown and it is often refractory to standard immunosuppression strategies, possibly leading to allograft loss. Here, we report a case of chronic active T-cell-mediated rejection caused by PCAR 12 years after kidney transplantation.</p><p><strong>Case presentation: </strong>A patient first visited our outpatient clinic with hematuria and proteinuria at the age of 23. He was followed as an outpatient for suspected chronic glomerulonephritis, but his kidney function gradually deteriorated and hemodialysis was initiated at age 50. ABO-compatible kidney transplantation was performed at 51. His graft function was stable for 11 years post-transplant with a serum level of creatinine of 1.5 mg/dL. Twelve years post-transplant, however, his graft function worsened to a creatinine level of 3.2 mg/dL, and he was admitted to our hospital for an allograft biopsy. The histopathology showed edematous lesions with massive tubulointerstitial plasma cell infiltration, and severe tubulitis, consistent with chronic active T-cell-mediated rejection type 1B according to the Banff classification 2019. He was treated with steroid pulse therapy (methylprednisolone 1,000 mg for 3 consecutive days), and his graft function improved to a creatinine level of 2.2 mg/dL. A repeat allograft biopsy 3 months after the steroid therapy showed improved interstitial edema and tubulitis.</p><p><strong>Conclusion: </strong>As suggested in this case, it is still possible to achieve a favorable response by initiating appropriate treatment in early stages of PCAR.</p>","PeriodicalId":9599,"journal":{"name":"Case Reports in Nephrology and Dialysis","volume":"15 1","pages":"206-215"},"PeriodicalIF":0.9000,"publicationDate":"2025-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12503644/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Case of Chronic Active T-Cell-Mediated Rejection Caused by Plasma Cell-Rich Acute Rejection 12 Years after Kidney Transplantation.\",\"authors\":\"Ayaka Hayashi, Izumi Yamamoto, Mayuko Kawabe, Yutaro Ohki, Akimitsu Kobayashi, Fumihiko Urabe, Takafumi Yanagisawa, Shunsuke Tsuzuki, Jun Miki, Takahiro Kimura, Ichiro Ohkido, Nobuo Tsuboi, Hiroyasu Yamamoto, Takashi Yokoo\",\"doi\":\"10.1159/000547828\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Plasma cell rich-acute rejection (PCAR) is a variant of T-cell-mediated rejection in kidney transplantation. Its pathogenesis remains unknown and it is often refractory to standard immunosuppression strategies, possibly leading to allograft loss. Here, we report a case of chronic active T-cell-mediated rejection caused by PCAR 12 years after kidney transplantation.</p><p><strong>Case presentation: </strong>A patient first visited our outpatient clinic with hematuria and proteinuria at the age of 23. He was followed as an outpatient for suspected chronic glomerulonephritis, but his kidney function gradually deteriorated and hemodialysis was initiated at age 50. ABO-compatible kidney transplantation was performed at 51. His graft function was stable for 11 years post-transplant with a serum level of creatinine of 1.5 mg/dL. Twelve years post-transplant, however, his graft function worsened to a creatinine level of 3.2 mg/dL, and he was admitted to our hospital for an allograft biopsy. The histopathology showed edematous lesions with massive tubulointerstitial plasma cell infiltration, and severe tubulitis, consistent with chronic active T-cell-mediated rejection type 1B according to the Banff classification 2019. He was treated with steroid pulse therapy (methylprednisolone 1,000 mg for 3 consecutive days), and his graft function improved to a creatinine level of 2.2 mg/dL. A repeat allograft biopsy 3 months after the steroid therapy showed improved interstitial edema and tubulitis.</p><p><strong>Conclusion: </strong>As suggested in this case, it is still possible to achieve a favorable response by initiating appropriate treatment in early stages of PCAR.</p>\",\"PeriodicalId\":9599,\"journal\":{\"name\":\"Case Reports in Nephrology and Dialysis\",\"volume\":\"15 1\",\"pages\":\"206-215\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-08-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12503644/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Nephrology and Dialysis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000547828\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology and Dialysis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000547828","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
A Case of Chronic Active T-Cell-Mediated Rejection Caused by Plasma Cell-Rich Acute Rejection 12 Years after Kidney Transplantation.
Introduction: Plasma cell rich-acute rejection (PCAR) is a variant of T-cell-mediated rejection in kidney transplantation. Its pathogenesis remains unknown and it is often refractory to standard immunosuppression strategies, possibly leading to allograft loss. Here, we report a case of chronic active T-cell-mediated rejection caused by PCAR 12 years after kidney transplantation.
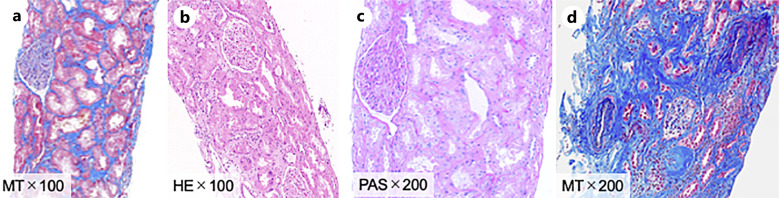
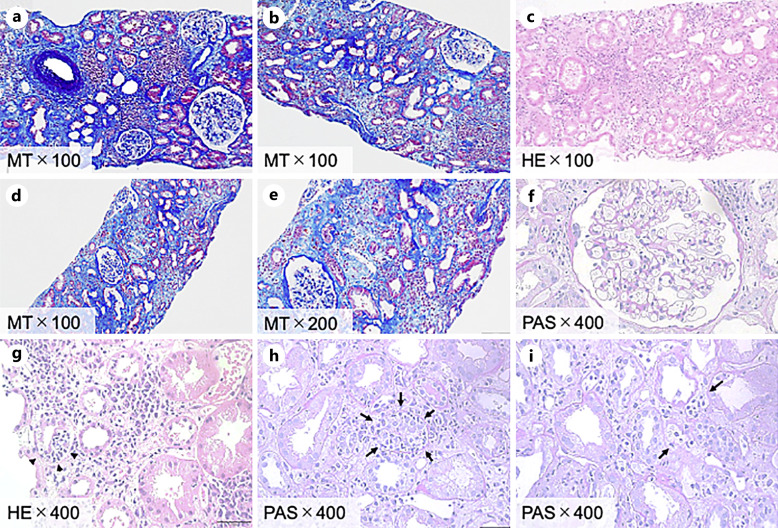
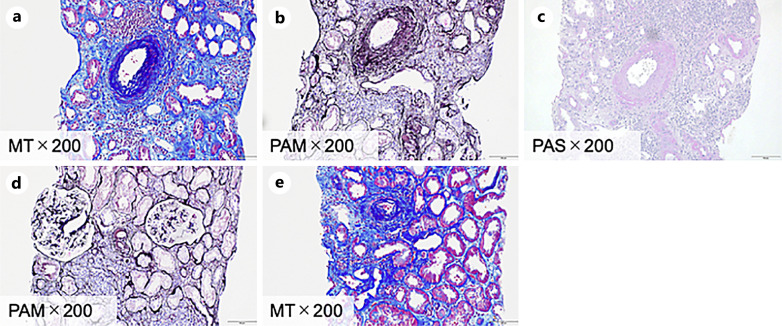
Case presentation: A patient first visited our outpatient clinic with hematuria and proteinuria at the age of 23. He was followed as an outpatient for suspected chronic glomerulonephritis, but his kidney function gradually deteriorated and hemodialysis was initiated at age 50. ABO-compatible kidney transplantation was performed at 51. His graft function was stable for 11 years post-transplant with a serum level of creatinine of 1.5 mg/dL. Twelve years post-transplant, however, his graft function worsened to a creatinine level of 3.2 mg/dL, and he was admitted to our hospital for an allograft biopsy. The histopathology showed edematous lesions with massive tubulointerstitial plasma cell infiltration, and severe tubulitis, consistent with chronic active T-cell-mediated rejection type 1B according to the Banff classification 2019. He was treated with steroid pulse therapy (methylprednisolone 1,000 mg for 3 consecutive days), and his graft function improved to a creatinine level of 2.2 mg/dL. A repeat allograft biopsy 3 months after the steroid therapy showed improved interstitial edema and tubulitis.
Conclusion: As suggested in this case, it is still possible to achieve a favorable response by initiating appropriate treatment in early stages of PCAR.
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of nephrology and dialysis, including genetic susceptibility, clinical presentation, diagnosis, treatment or prevention, toxicities of therapy, critical care, supportive care, quality-of-life and survival issues. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


