Leon M Bischoff, Sebastian Nowak, Maximilian Mader, Maike Theis, Thomas Vollbrecht, Alexander Isaak, Daniel Kuetting, Claus C Pieper, Annegret Geipel, Florian Kipfmueller, Brigitte Strizek, Alois M Sprinkart, Julian A Luetkens
{"title":"先天性膈疝的胎儿MRI深度学习分割。","authors":"Leon M Bischoff, Sebastian Nowak, Maximilian Mader, Maike Theis, Thomas Vollbrecht, Alexander Isaak, Daniel Kuetting, Claus C Pieper, Annegret Geipel, Florian Kipfmueller, Brigitte Strizek, Alois M Sprinkart, Julian A Luetkens","doi":"10.1093/radadv/umae034","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To determine if deep learning (DL) segmentation of total fetal body volume (TFBV) and total fetal lung volume (TFLV) in fetuses with congenital diaphragmatic hernia has comparable performance to manual segmentation.</p><p><strong>Materials and methods: </strong>A total of 208 fetal MRI studies with congenital diaphragmatic hernia, acquired between August 2007 and September 2023, were retrospectively included. TFBV and TFLV were extracted from manual tissue segmentations in balanced gradient echo and single shot T2-weighted turbo spin echo sequences. MRI studies were split into training (n = 188) and hold-out test data (n = 20). Wilcoxon signed-rank test was used to compare manual and DL-based segmentations by 2 U-Nets. Manual and DL segmentation times were noted and compared using Student's t-test. The observed/expected ratio of the total lung volume (O/E TLV) as a prognostic marker for postnatal survival was calculated. Outcome predictions of O/E TLV for postnatal death were assessed with univariate regression analysis.</p><p><strong>Results: </strong>Manual segmentation times were higher compared to DL segmentations (30 ± 7 minutes versus 0.25 ± 0.05 minutes, <i>P </i><<i> </i>.001). Manual and DL-based TFBV were similar (1317 ± 498 mL versus 1306 ± 491 mL; <i>P</i> = .04; Dice score: 0.98 ± 0.01). TFLV (19.4 ± 11.5 mL versus 18.7 ± 12.4 mL; <i>P = </i>.11; Dice score: 0.84 ± 0.09) and O/E TLV (39.3 ± 18.1 mL versus 37.7 ± 19.1 mL, <i>P = </i>.13) were not significantly different. Postnatal mortality was negatively associated with higher manual O/E TLV (odds ratio: 0.97; 95% confidence interval [CI], 0.96-0.98; <i>P </i><<i> </i>.001) and DL O/E TLV (odds ratio: 0.97; 95% CI, 0.96-0.98; <i>P </i><<i> </i>.001).</p><p><strong>Conclusion: </strong>DL for body and lung segmentation in fetuses with congenital diaphragmatic hernia allows reliable and rapid calculations of the observed/expected ratio and equally predicts prognostic outcome.</p>","PeriodicalId":519940,"journal":{"name":"Radiology advances","volume":"2 1","pages":"umae034"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12429181/pdf/","citationCount":"0","resultStr":"{\"title\":\"Fetal MRI deep learning segmentation of body and lung in congenital diaphragmatic hernia.\",\"authors\":\"Leon M Bischoff, Sebastian Nowak, Maximilian Mader, Maike Theis, Thomas Vollbrecht, Alexander Isaak, Daniel Kuetting, Claus C Pieper, Annegret Geipel, Florian Kipfmueller, Brigitte Strizek, Alois M Sprinkart, Julian A Luetkens\",\"doi\":\"10.1093/radadv/umae034\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To determine if deep learning (DL) segmentation of total fetal body volume (TFBV) and total fetal lung volume (TFLV) in fetuses with congenital diaphragmatic hernia has comparable performance to manual segmentation.</p><p><strong>Materials and methods: </strong>A total of 208 fetal MRI studies with congenital diaphragmatic hernia, acquired between August 2007 and September 2023, were retrospectively included. TFBV and TFLV were extracted from manual tissue segmentations in balanced gradient echo and single shot T2-weighted turbo spin echo sequences. MRI studies were split into training (n = 188) and hold-out test data (n = 20). Wilcoxon signed-rank test was used to compare manual and DL-based segmentations by 2 U-Nets. Manual and DL segmentation times were noted and compared using Student's t-test. The observed/expected ratio of the total lung volume (O/E TLV) as a prognostic marker for postnatal survival was calculated. Outcome predictions of O/E TLV for postnatal death were assessed with univariate regression analysis.</p><p><strong>Results: </strong>Manual segmentation times were higher compared to DL segmentations (30 ± 7 minutes versus 0.25 ± 0.05 minutes, <i>P </i><<i> </i>.001). Manual and DL-based TFBV were similar (1317 ± 498 mL versus 1306 ± 491 mL; <i>P</i> = .04; Dice score: 0.98 ± 0.01). TFLV (19.4 ± 11.5 mL versus 18.7 ± 12.4 mL; <i>P = </i>.11; Dice score: 0.84 ± 0.09) and O/E TLV (39.3 ± 18.1 mL versus 37.7 ± 19.1 mL, <i>P = </i>.13) were not significantly different. Postnatal mortality was negatively associated with higher manual O/E TLV (odds ratio: 0.97; 95% confidence interval [CI], 0.96-0.98; <i>P </i><<i> </i>.001) and DL O/E TLV (odds ratio: 0.97; 95% CI, 0.96-0.98; <i>P </i><<i> </i>.001).</p><p><strong>Conclusion: </strong>DL for body and lung segmentation in fetuses with congenital diaphragmatic hernia allows reliable and rapid calculations of the observed/expected ratio and equally predicts prognostic outcome.</p>\",\"PeriodicalId\":519940,\"journal\":{\"name\":\"Radiology advances\",\"volume\":\"2 1\",\"pages\":\"umae034\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-12-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12429181/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiology advances\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/radadv/umae034\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiology advances","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/radadv/umae034","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:探讨深度学习(DL)分割先天性膈疝胎儿的总胎体体积(TFBV)和总胎肺体积(TFLV)是否与手工分割具有可比性。材料和方法:回顾性分析2007年8月至2023年9月期间获得的208例先天性膈疝胎儿MRI研究。在平衡梯度回波和单次t2加权涡轮自旋回波序列中提取人工组织分割的TFBV和TFLV。MRI研究分为训练数据(n = 188)和保留测试数据(n = 20)。使用Wilcoxon符号秩检验比较2个U-Nets的人工和基于dl的分割。使用学生t检验记录和比较手工和DL分割时间。计算肺总容积(O/E TLV)的观察/预期比,作为产后生存的预后指标。采用单因素回归分析评估O/E TLV对产后死亡的预后预测。结果:人工分割时间比深度分割时间长(30±7分钟vs 0.25±0.05分钟,P .001)。手动TFBV与基于dl的TFBV相似(1317±498 mL vs 1306±491 mL; P = 0.04; Dice评分:0.98±0.01)。TFLV(19.4±11.5毫升和18.7±12.4毫升;P =厚;骰子得分:0.84±0.09)和O / E电磁阀(39.3±18.1毫升和37.7±19.1毫升,P =。13)无显著差异。产后死亡率与较高的人工O/E TLV呈负相关(优势比:0.97;95%可信区间[CI], 0.96-0.98; P。001)和DL O/E TLV(优势比:0.97;95% CI, 0.96-0.98; P .001)。结论:先天性膈疝胎儿的身体和肺分割DL可以可靠、快速地计算观察/预期比率,并同样预测预后结果。
Fetal MRI deep learning segmentation of body and lung in congenital diaphragmatic hernia.
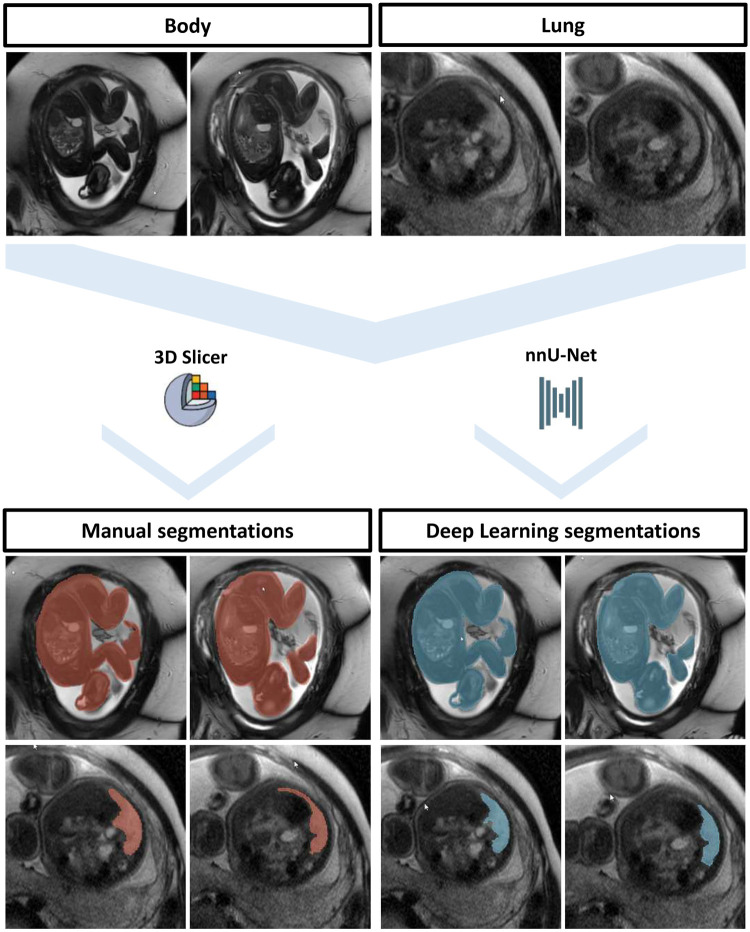
Purpose: To determine if deep learning (DL) segmentation of total fetal body volume (TFBV) and total fetal lung volume (TFLV) in fetuses with congenital diaphragmatic hernia has comparable performance to manual segmentation.
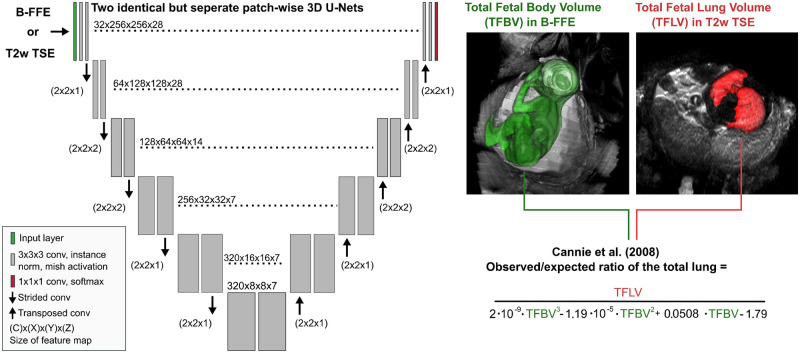
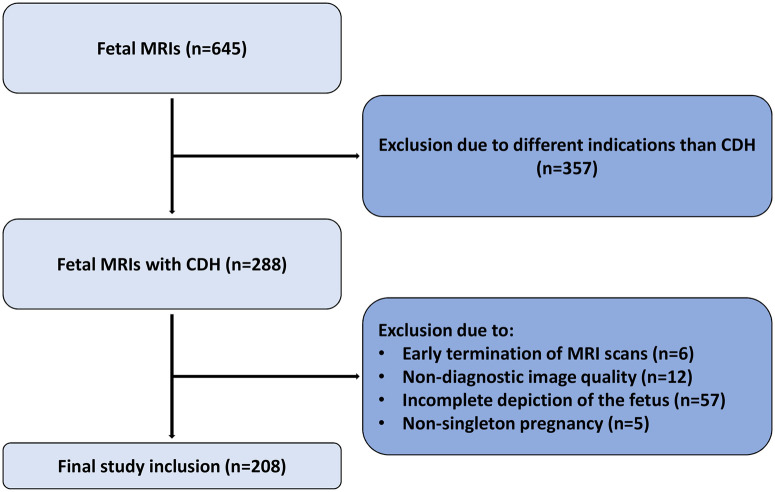
Materials and methods: A total of 208 fetal MRI studies with congenital diaphragmatic hernia, acquired between August 2007 and September 2023, were retrospectively included. TFBV and TFLV were extracted from manual tissue segmentations in balanced gradient echo and single shot T2-weighted turbo spin echo sequences. MRI studies were split into training (n = 188) and hold-out test data (n = 20). Wilcoxon signed-rank test was used to compare manual and DL-based segmentations by 2 U-Nets. Manual and DL segmentation times were noted and compared using Student's t-test. The observed/expected ratio of the total lung volume (O/E TLV) as a prognostic marker for postnatal survival was calculated. Outcome predictions of O/E TLV for postnatal death were assessed with univariate regression analysis.
Results: Manual segmentation times were higher compared to DL segmentations (30 ± 7 minutes versus 0.25 ± 0.05 minutes, P <.001). Manual and DL-based TFBV were similar (1317 ± 498 mL versus 1306 ± 491 mL; P = .04; Dice score: 0.98 ± 0.01). TFLV (19.4 ± 11.5 mL versus 18.7 ± 12.4 mL; P = .11; Dice score: 0.84 ± 0.09) and O/E TLV (39.3 ± 18.1 mL versus 37.7 ± 19.1 mL, P = .13) were not significantly different. Postnatal mortality was negatively associated with higher manual O/E TLV (odds ratio: 0.97; 95% confidence interval [CI], 0.96-0.98; P <.001) and DL O/E TLV (odds ratio: 0.97; 95% CI, 0.96-0.98; P <.001).
Conclusion: DL for body and lung segmentation in fetuses with congenital diaphragmatic hernia allows reliable and rapid calculations of the observed/expected ratio and equally predicts prognostic outcome.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


