Jackie Robinson, Bert van der Werf, Daniel Exeter, Jinfeng Zhao, Merryn Gott
{"title":"地区贫困对生命最后一年获得和利用保健服务的影响:一项基于人口的回顾性队列研究。","authors":"Jackie Robinson, Bert van der Werf, Daniel Exeter, Jinfeng Zhao, Merryn Gott","doi":"10.1177/26323524251332302","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The healthcare needs of people living in areas of high deprivation are complicated by the cumulative effect of the sociodemographic factors known to impact on health outcomes, such as income, housing and education. Of note, for people living in more deprived areas, life expectancy is shorter and the onset of chronic disease and multimorbidity occurs much earlier. While the relationship between area deprivation and access to palliative care is becoming more widely researched, the vast majority of studies to date have focused on referrals to specialist palliative care services. This is problematic given the dominant model of generalist-specialist palliative care in high-income countries which assumes that most people will have a level of palliative care need that can be managed by non-specialist palliative care services.</p><p><strong>Objective: </strong>To identify associations between area deprivation and the use of generalist and specialist palliative care services in the last year of life.</p><p><strong>Design: </strong>A retrospective population-based cohort study.</p><p><strong>Methods: </strong>People aged over 18 years who died between January 2015 and December 2020 were identified within one geographical area of Aotearoa New Zealand. Using the National Health Identifier, deaths were matched to generalist and specialist palliative care service data.</p><p><strong>Results: </strong>A significant association was found between area deprivation and health service use in the last year of life. Of note, people living in rural areas of deprivation were significantly less likely to receive a hospital (<i>p</i> = <0.000) or inpatient hospice admission (<i>p</i> = <0.000). They were also less likely to have contact with their general practitioner (<i>p</i> = 0.007) or experience a specialist outpatient clinic appointment (<i>p</i> = 0.001).</p><p><strong>Conclusion: </strong>This study has revealed inequities in health service use across generalist and specialist palliative care services for people living in areas of deprivation. Of note, findings have highlighted how rurality amplifies inequities in access to appropriate palliative care. Further research is needed to better understand the consequences of these apparent inequities.</p>","PeriodicalId":36693,"journal":{"name":"Palliative Care and Social Practice","volume":"19 ","pages":"26323524251332302"},"PeriodicalIF":2.2000,"publicationDate":"2025-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12497965/pdf/","citationCount":"0","resultStr":"{\"title\":\"The impact of area deprivation on access to and utilization of health services in the last year of life: A retrospective population-based cohort study.\",\"authors\":\"Jackie Robinson, Bert van der Werf, Daniel Exeter, Jinfeng Zhao, Merryn Gott\",\"doi\":\"10.1177/26323524251332302\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The healthcare needs of people living in areas of high deprivation are complicated by the cumulative effect of the sociodemographic factors known to impact on health outcomes, such as income, housing and education. Of note, for people living in more deprived areas, life expectancy is shorter and the onset of chronic disease and multimorbidity occurs much earlier. While the relationship between area deprivation and access to palliative care is becoming more widely researched, the vast majority of studies to date have focused on referrals to specialist palliative care services. This is problematic given the dominant model of generalist-specialist palliative care in high-income countries which assumes that most people will have a level of palliative care need that can be managed by non-specialist palliative care services.</p><p><strong>Objective: </strong>To identify associations between area deprivation and the use of generalist and specialist palliative care services in the last year of life.</p><p><strong>Design: </strong>A retrospective population-based cohort study.</p><p><strong>Methods: </strong>People aged over 18 years who died between January 2015 and December 2020 were identified within one geographical area of Aotearoa New Zealand. Using the National Health Identifier, deaths were matched to generalist and specialist palliative care service data.</p><p><strong>Results: </strong>A significant association was found between area deprivation and health service use in the last year of life. Of note, people living in rural areas of deprivation were significantly less likely to receive a hospital (<i>p</i> = <0.000) or inpatient hospice admission (<i>p</i> = <0.000). They were also less likely to have contact with their general practitioner (<i>p</i> = 0.007) or experience a specialist outpatient clinic appointment (<i>p</i> = 0.001).</p><p><strong>Conclusion: </strong>This study has revealed inequities in health service use across generalist and specialist palliative care services for people living in areas of deprivation. Of note, findings have highlighted how rurality amplifies inequities in access to appropriate palliative care. Further research is needed to better understand the consequences of these apparent inequities.</p>\",\"PeriodicalId\":36693,\"journal\":{\"name\":\"Palliative Care and Social Practice\",\"volume\":\"19 \",\"pages\":\"26323524251332302\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-10-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12497965/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Palliative Care and Social Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/26323524251332302\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative Care and Social Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26323524251332302","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
摘要
背景:生活在高度贫困地区的人们的保健需求因已知影响健康结果的社会人口因素(如收入、住房和教育)的累积效应而变得复杂。值得注意的是,对于生活在较贫困地区的人来说,预期寿命较短,慢性病和多种疾病的发病要早得多。虽然区域剥夺与获得姑息治疗之间的关系正在得到越来越广泛的研究,但迄今为止绝大多数研究都集中在转诊到专科姑息治疗服务上。鉴于高收入国家的全科-专科姑息治疗占主导地位的模式,这是有问题的,这种模式假定大多数人将有一定程度的姑息治疗需求,可以通过非专科姑息治疗服务来管理。目的:确定在生命的最后一年,区域剥夺和使用全科和专科姑息治疗服务之间的联系。设计:一项基于人群的回顾性队列研究。方法:选取2015年1月至2020年12月期间在新西兰奥特罗阿一个地理区域内死亡的18岁以上人群。使用国家健康标识符,将死亡与全科和专科姑息治疗服务数据相匹配。结果:区域剥夺与生命最后一年的卫生服务使用之间存在显著关联。值得注意的是,生活在贫困农村地区的人接受医院治疗(p = p = p = 0.007)或接受专科门诊预约(p = 0.001)的可能性明显较低。结论:这项研究揭示了生活在贫困地区的人们在医疗服务使用方面的不公平现象,包括全科和专科姑息治疗服务。值得注意的是,调查结果强调了农村如何加剧了在获得适当姑息治疗方面的不平等。为了更好地理解这些明显的不平等的后果,需要进一步的研究。
The impact of area deprivation on access to and utilization of health services in the last year of life: A retrospective population-based cohort study.
Background: The healthcare needs of people living in areas of high deprivation are complicated by the cumulative effect of the sociodemographic factors known to impact on health outcomes, such as income, housing and education. Of note, for people living in more deprived areas, life expectancy is shorter and the onset of chronic disease and multimorbidity occurs much earlier. While the relationship between area deprivation and access to palliative care is becoming more widely researched, the vast majority of studies to date have focused on referrals to specialist palliative care services. This is problematic given the dominant model of generalist-specialist palliative care in high-income countries which assumes that most people will have a level of palliative care need that can be managed by non-specialist palliative care services.
Objective: To identify associations between area deprivation and the use of generalist and specialist palliative care services in the last year of life.
Design: A retrospective population-based cohort study.
Methods: People aged over 18 years who died between January 2015 and December 2020 were identified within one geographical area of Aotearoa New Zealand. Using the National Health Identifier, deaths were matched to generalist and specialist palliative care service data.
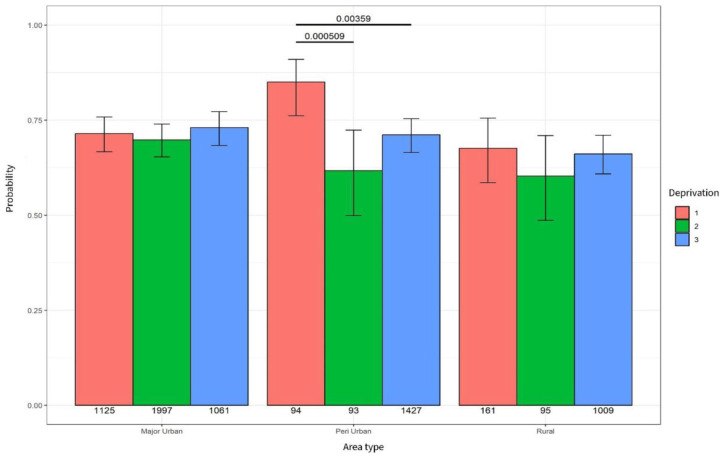
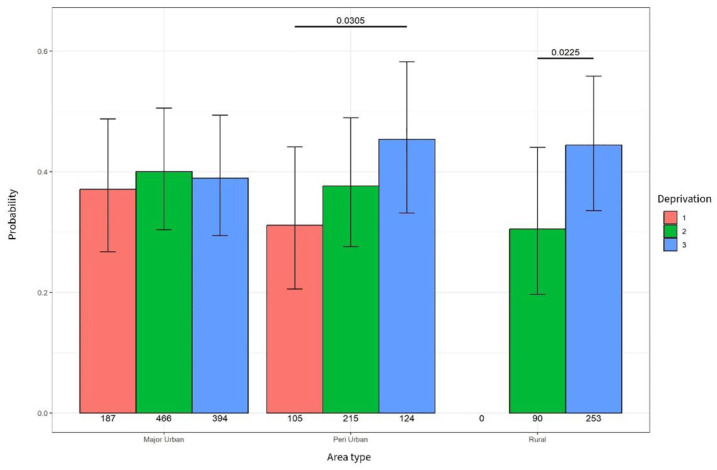
Results: A significant association was found between area deprivation and health service use in the last year of life. Of note, people living in rural areas of deprivation were significantly less likely to receive a hospital (p = <0.000) or inpatient hospice admission (p = <0.000). They were also less likely to have contact with their general practitioner (p = 0.007) or experience a specialist outpatient clinic appointment (p = 0.001).
Conclusion: This study has revealed inequities in health service use across generalist and specialist palliative care services for people living in areas of deprivation. Of note, findings have highlighted how rurality amplifies inequities in access to appropriate palliative care. Further research is needed to better understand the consequences of these apparent inequities.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


