Hashim J F Shaikh, Michaela L Malin, Andrew Jeong, Devon E Anderson, Gregg T Nicandri, Brian D Giordano, Ilya Voloshin, Michael D Maloney, Sandeep Mannava
{"title":"在接受关节镜下肩袖修复的患者中,伴随的颈椎疾病恶化了预后。","authors":"Hashim J F Shaikh, Michaela L Malin, Andrew Jeong, Devon E Anderson, Gregg T Nicandri, Brian D Giordano, Ilya Voloshin, Michael D Maloney, Sandeep Mannava","doi":"10.1177/23259671251372618","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rotator cuff disease is one of the most common causes of shoulder disability. Pathologic conditions of the shoulder are often complicated by concomitant conditions such as cervical spine (C-spine) disease.</p><p><strong>Purpose/hypothesis: </strong>The purpose of this article is to assess whether patients with concomitant C-spine disease undergoing arthroscopic rotator cuff repair (ARCR) demonstrate lower absolute values in Patient-Reported Outcomes Measurement Information System (PROMIS) scores compared with those without C-spine disease and whether it affects the achievement of the minimal clinically important difference (MCID). It was hypothesized that patients with C-spine disease undergoing ARCR demonstrate lower absolute values in PROMIS scores compared with those without concomitant C-spine disease, but those patients experience a similar improvement and achievement of MCID after ARCR surgery.</p><p><strong>Study design: </strong>Cohort study; Level of evidence, 3.</p><p><strong>Methods: </strong>A total of 1387 patients who underwent ARCR at a single institution were identified. A retrospective chart review of a prospectively collected database was conducted to capture PROMIS Pain Interference (PI), Physical Function (PF), and Depression (Dep) scores. Patients were stratified into 2 groups based on the presence of concomitant C-spine disease at the time of surgery. The MCID was calculated using a distribution-based methodology.</p><p><strong>Results: </strong>Of the total, 528 patients met inclusion criteria for final analysis, 120 of whom had concomitant C-spine disease. Unadjusted analysis of descriptive variables revealed no significant differences between the C-spine and control groups. Both cohorts showed significant improvement at final follow-up compared with their preoperative PROMIS values for PF, PI, and Dep (<i>P</i> < .001). Compared with patients without it, those with concomitant C-spine disease had statistically worse preoperative PROMIS scores for PI (62.6 ± 6.8 vs 60.1 ± 6.8; <i>P</i> = .001), Dep (50.4 ± 9.8 vs 47.6 ± 9.8; <i>P</i> = .004), and PF scores (39.5 ± 7.3 vs 42.6 ± 8.4; <i>P</i> = .001), as well as worse postoperative scores for PI (53.9 ± 7.9 vs 50.5 ± 8.1; <i>P</i> = .001), Dep (43.4 ± 9.4 vs 41.1 ± 7.8; <i>P</i> = .003), and PF (45.6 ± 7.6 vs 48.6 ± 7.9; <i>P</i> = .001). Notably, these differences while statistically significant were not clinically significant due to the overlap between the C-spine and control group PROMIS scores in each domain. No significant difference was found in the achievement of MCID between the 2 groups for PF, PI, or Dep. Regression analysis revealed that C-spine disease was not a significant predictor of achievement of MCID in any of the 3 PROMIS domains.</p><p><strong>Conclusion: </strong>This study underscores the broad applicability of ARCR for patients with complex musculoskeletal pathology such as concomitant C-spine disease. The findings highlight the importance of setting expectations for patients regardless of their concomitant C-spine pathology before surgery.</p>","PeriodicalId":19646,"journal":{"name":"Orthopaedic Journal of Sports Medicine","volume":"13 10","pages":"23259671251372618"},"PeriodicalIF":2.5000,"publicationDate":"2025-10-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12495215/pdf/","citationCount":"0","resultStr":"{\"title\":\"Concomitant Cervical Spine Disease Worsens PROMIS Outcomes in Patients Undergoing Arthroscopic Rotator Cuff Repair.\",\"authors\":\"Hashim J F Shaikh, Michaela L Malin, Andrew Jeong, Devon E Anderson, Gregg T Nicandri, Brian D Giordano, Ilya Voloshin, Michael D Maloney, Sandeep Mannava\",\"doi\":\"10.1177/23259671251372618\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Rotator cuff disease is one of the most common causes of shoulder disability. Pathologic conditions of the shoulder are often complicated by concomitant conditions such as cervical spine (C-spine) disease.</p><p><strong>Purpose/hypothesis: </strong>The purpose of this article is to assess whether patients with concomitant C-spine disease undergoing arthroscopic rotator cuff repair (ARCR) demonstrate lower absolute values in Patient-Reported Outcomes Measurement Information System (PROMIS) scores compared with those without C-spine disease and whether it affects the achievement of the minimal clinically important difference (MCID). It was hypothesized that patients with C-spine disease undergoing ARCR demonstrate lower absolute values in PROMIS scores compared with those without concomitant C-spine disease, but those patients experience a similar improvement and achievement of MCID after ARCR surgery.</p><p><strong>Study design: </strong>Cohort study; Level of evidence, 3.</p><p><strong>Methods: </strong>A total of 1387 patients who underwent ARCR at a single institution were identified. A retrospective chart review of a prospectively collected database was conducted to capture PROMIS Pain Interference (PI), Physical Function (PF), and Depression (Dep) scores. Patients were stratified into 2 groups based on the presence of concomitant C-spine disease at the time of surgery. The MCID was calculated using a distribution-based methodology.</p><p><strong>Results: </strong>Of the total, 528 patients met inclusion criteria for final analysis, 120 of whom had concomitant C-spine disease. Unadjusted analysis of descriptive variables revealed no significant differences between the C-spine and control groups. Both cohorts showed significant improvement at final follow-up compared with their preoperative PROMIS values for PF, PI, and Dep (<i>P</i> < .001). Compared with patients without it, those with concomitant C-spine disease had statistically worse preoperative PROMIS scores for PI (62.6 ± 6.8 vs 60.1 ± 6.8; <i>P</i> = .001), Dep (50.4 ± 9.8 vs 47.6 ± 9.8; <i>P</i> = .004), and PF scores (39.5 ± 7.3 vs 42.6 ± 8.4; <i>P</i> = .001), as well as worse postoperative scores for PI (53.9 ± 7.9 vs 50.5 ± 8.1; <i>P</i> = .001), Dep (43.4 ± 9.4 vs 41.1 ± 7.8; <i>P</i> = .003), and PF (45.6 ± 7.6 vs 48.6 ± 7.9; <i>P</i> = .001). Notably, these differences while statistically significant were not clinically significant due to the overlap between the C-spine and control group PROMIS scores in each domain. No significant difference was found in the achievement of MCID between the 2 groups for PF, PI, or Dep. Regression analysis revealed that C-spine disease was not a significant predictor of achievement of MCID in any of the 3 PROMIS domains.</p><p><strong>Conclusion: </strong>This study underscores the broad applicability of ARCR for patients with complex musculoskeletal pathology such as concomitant C-spine disease. The findings highlight the importance of setting expectations for patients regardless of their concomitant C-spine pathology before surgery.</p>\",\"PeriodicalId\":19646,\"journal\":{\"name\":\"Orthopaedic Journal of Sports Medicine\",\"volume\":\"13 10\",\"pages\":\"23259671251372618\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-10-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12495215/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Orthopaedic Journal of Sports Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/23259671251372618\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Orthopaedic Journal of Sports Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/23259671251372618","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:肩袖疾病是导致肩部残疾的最常见原因之一。肩关节的病理状况常伴有诸如颈椎(C-spine)疾病等并发症。目的/假设:本文的目的是评估接受关节镜下肩袖修复术(ARCR)的伴有颈椎疾病的患者在患者报告结果测量信息系统(PROMIS)评分中的绝对值是否低于无颈椎疾病的患者,以及这是否影响最小临床重要差异(MCID)的实现。假设接受ARCR的c -脊柱疾病患者的PROMIS评分的绝对值比没有合并c -脊柱疾病的患者低,但这些患者在ARCR手术后的MCID改善和成就相似。研究设计:队列研究;证据水平,3。方法:在单一机构共确定了1387例接受ARCR的患者。对前瞻性收集的数据库进行回顾性图表回顾,以获取PROMIS疼痛干扰(PI)、身体功能(PF)和抑郁(Dep)评分。根据手术时是否伴有颈椎疾病将患者分为两组。MCID采用基于分布的方法计算。结果:528例患者符合最终分析的纳入标准,其中120例合并了颈椎疾病。未经调整的描述性变量分析显示,在c -脊柱组和对照组之间没有显著差异。两组患者在最终随访时均较术前PF、PI和Dep的PROMIS值有显著改善(P < 0.001)。与病人没有它相比,那些伴随C-spine疾病术前PROMIS分数统计更糟了π(62.6±6.8 vs 60.1±6.8;P =措施),大(50.4±9.8 vs 47.6±9.8;P = 04),和PF成绩(39.5±7.3 vs 42.6±8.4;P =措施),以及更糟糕的是术后分数π(53.9±7.9 vs 50.5±8.1;P =措施),大(43.4±9.4 vs 41.1±7.8;P = .003),和PF(45.6±7.6 vs 48.6±7.9;P =措施)。值得注意的是,这些差异虽然具有统计学意义,但没有临床意义,因为c -脊柱组和对照组在各领域的PROMIS评分存在重叠。两组在PF、PI或Dep的MCID成就方面没有发现显著差异。回归分析显示,在任何3个PROMIS域中,颈椎疾病都不是MCID成就的显著预测因子。结论:本研究强调了ARCR在复杂肌肉骨骼病理(如合并颈椎疾病)患者中的广泛适用性。研究结果强调了术前对患者设定期望的重要性,而不考虑其伴随的颈椎病理。
Background: Rotator cuff disease is one of the most common causes of shoulder disability. Pathologic conditions of the shoulder are often complicated by concomitant conditions such as cervical spine (C-spine) disease.
Purpose/hypothesis: The purpose of this article is to assess whether patients with concomitant C-spine disease undergoing arthroscopic rotator cuff repair (ARCR) demonstrate lower absolute values in Patient-Reported Outcomes Measurement Information System (PROMIS) scores compared with those without C-spine disease and whether it affects the achievement of the minimal clinically important difference (MCID). It was hypothesized that patients with C-spine disease undergoing ARCR demonstrate lower absolute values in PROMIS scores compared with those without concomitant C-spine disease, but those patients experience a similar improvement and achievement of MCID after ARCR surgery.
Study design: Cohort study; Level of evidence, 3.
Methods: A total of 1387 patients who underwent ARCR at a single institution were identified. A retrospective chart review of a prospectively collected database was conducted to capture PROMIS Pain Interference (PI), Physical Function (PF), and Depression (Dep) scores. Patients were stratified into 2 groups based on the presence of concomitant C-spine disease at the time of surgery. The MCID was calculated using a distribution-based methodology.
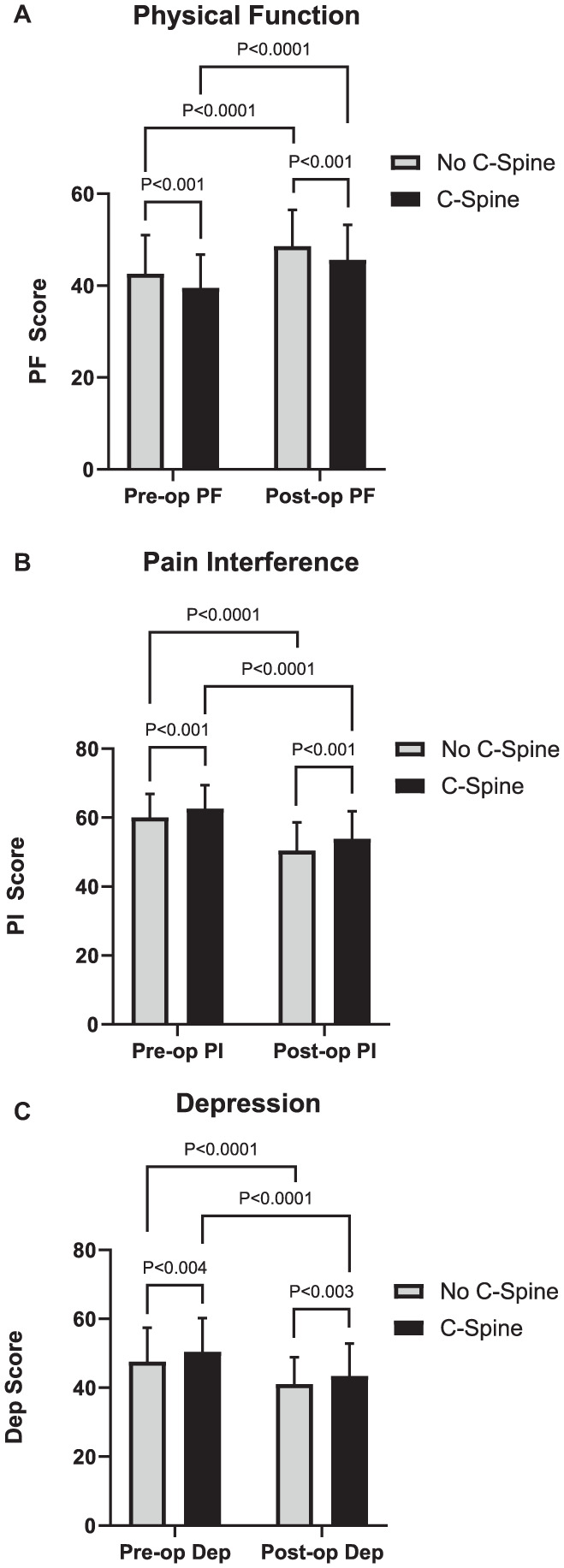
Results: Of the total, 528 patients met inclusion criteria for final analysis, 120 of whom had concomitant C-spine disease. Unadjusted analysis of descriptive variables revealed no significant differences between the C-spine and control groups. Both cohorts showed significant improvement at final follow-up compared with their preoperative PROMIS values for PF, PI, and Dep (P < .001). Compared with patients without it, those with concomitant C-spine disease had statistically worse preoperative PROMIS scores for PI (62.6 ± 6.8 vs 60.1 ± 6.8; P = .001), Dep (50.4 ± 9.8 vs 47.6 ± 9.8; P = .004), and PF scores (39.5 ± 7.3 vs 42.6 ± 8.4; P = .001), as well as worse postoperative scores for PI (53.9 ± 7.9 vs 50.5 ± 8.1; P = .001), Dep (43.4 ± 9.4 vs 41.1 ± 7.8; P = .003), and PF (45.6 ± 7.6 vs 48.6 ± 7.9; P = .001). Notably, these differences while statistically significant were not clinically significant due to the overlap between the C-spine and control group PROMIS scores in each domain. No significant difference was found in the achievement of MCID between the 2 groups for PF, PI, or Dep. Regression analysis revealed that C-spine disease was not a significant predictor of achievement of MCID in any of the 3 PROMIS domains.
Conclusion: This study underscores the broad applicability of ARCR for patients with complex musculoskeletal pathology such as concomitant C-spine disease. The findings highlight the importance of setting expectations for patients regardless of their concomitant C-spine pathology before surgery.
期刊介绍:
The Orthopaedic Journal of Sports Medicine (OJSM), developed by the American Orthopaedic Society for Sports Medicine (AOSSM), is a global, peer-reviewed, open access journal that combines the interests of researchers and clinical practitioners across orthopaedic sports medicine, arthroscopy, and knee arthroplasty.
Topics include original research in the areas of:
-Orthopaedic Sports Medicine, including surgical and nonsurgical treatment of orthopaedic sports injuries
-Arthroscopic Surgery (Shoulder/Elbow/Wrist/Hip/Knee/Ankle/Foot)
-Relevant translational research
-Sports traumatology/epidemiology
-Knee and shoulder arthroplasty
The OJSM also publishes relevant systematic reviews and meta-analyses.
This journal is a member of the Committee on Publication Ethics (COPE).


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


