{"title":"全静脉麻醉下进行食管胃十二指肠镜和结肠镜联合检查的高危患者并发症的发生率:一项前瞻性队列研究。","authors":"Wilaiporn Supan, Araya Ongiem, Papiroon Noitasaeng, Pathomporn Bunnag, Uayporn Kaosombatwattana, Orawan Supapueng, Phongthara Vichitvejpaisal","doi":"10.2147/TCRM.S541750","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the incidence, characteristics, and risk factors of complications related to anesthesia complication in ASA Class III patients undergoing combined esophagogastroduodenoscopy (EGD) and colonoscopy under total intravenous anesthesia (TIVA).</p><p><strong>Materials and methods: </strong>This prospective cohort study was conducted from April 1, 2024, to February 11, 2025. Data collected included baseline characteristics (age, sex, comorbidities, functional capacity, nutritional status, smoking, fasting and medications) and intraoperative/postoperative parameters (anesthetic technique, sedative dosing, IV fluids, complications, and 24-hour status). Descriptive statistics, univariate analysis, and binary logistic regression were applied.</p><p><strong>Results: </strong>Of 403 ASA Class III patients enrolled, 393 were analyzed after excluding 10 for inadequate bowel prep or early termination due to malignancy. A total of 207 patients (52.7%) experienced at least one complication. Common complications included transient hypotension (40.2%), desaturation (15.8%), and airway obstruction (15.5%). Less frequent events were bradycardia (4.1%), hypoxia (1.8%), hypertension (1.8%), tachycardia (0.3%) and respiratory depression (0.5%). Five independent risk factors were significantly associated with complications: preexisting cardiovascular disease - odds ratio (OR=1.678), respiratory disease (OR=1.877), functional capacity < 4 metabolic equivalents (METs), (OR=1.851), nutritional screening score ≥1 (OR =1.518), and single - dose bowel prep regimen (OR=1.614). Complications were more common in women, patients aged 65 years or older, and inpatients, although the difference in hospitalization and outpatient was not statistically significant. Patients with complications received lower total doses of propofol and fentanyl per weight per hour. Dexmedetomidine use was significantly associated with complications among inpatients (p = 0.015). The duration of the procedure was longer in patients with complications (p = 0.002).</p><p><strong>Conclusion: </strong>Anesthesia-related complications were frequent among ASA Class III patients who underwent combined EGD and colonoscopy under TIVA, particularly cardiovascular and respiratory events. Identification of five preprocedural risk factors supports the need for improved risk stratification and individualized sedation planning to optimize safety in this high-risk group.</p>","PeriodicalId":22977,"journal":{"name":"Therapeutics and Clinical Risk Management","volume":"21 ","pages":"1395-1408"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12485486/pdf/","citationCount":"0","resultStr":"{\"title\":\"Incidence of Complications in High-Risk Patients Undergoing Combined Esophagogastroduodenoscopy and Colonoscopy with Total Intravenous Anesthesia: A Prospective Cohort Study.\",\"authors\":\"Wilaiporn Supan, Araya Ongiem, Papiroon Noitasaeng, Pathomporn Bunnag, Uayporn Kaosombatwattana, Orawan Supapueng, Phongthara Vichitvejpaisal\",\"doi\":\"10.2147/TCRM.S541750\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To evaluate the incidence, characteristics, and risk factors of complications related to anesthesia complication in ASA Class III patients undergoing combined esophagogastroduodenoscopy (EGD) and colonoscopy under total intravenous anesthesia (TIVA).</p><p><strong>Materials and methods: </strong>This prospective cohort study was conducted from April 1, 2024, to February 11, 2025. Data collected included baseline characteristics (age, sex, comorbidities, functional capacity, nutritional status, smoking, fasting and medications) and intraoperative/postoperative parameters (anesthetic technique, sedative dosing, IV fluids, complications, and 24-hour status). Descriptive statistics, univariate analysis, and binary logistic regression were applied.</p><p><strong>Results: </strong>Of 403 ASA Class III patients enrolled, 393 were analyzed after excluding 10 for inadequate bowel prep or early termination due to malignancy. A total of 207 patients (52.7%) experienced at least one complication. Common complications included transient hypotension (40.2%), desaturation (15.8%), and airway obstruction (15.5%). Less frequent events were bradycardia (4.1%), hypoxia (1.8%), hypertension (1.8%), tachycardia (0.3%) and respiratory depression (0.5%). Five independent risk factors were significantly associated with complications: preexisting cardiovascular disease - odds ratio (OR=1.678), respiratory disease (OR=1.877), functional capacity < 4 metabolic equivalents (METs), (OR=1.851), nutritional screening score ≥1 (OR =1.518), and single - dose bowel prep regimen (OR=1.614). Complications were more common in women, patients aged 65 years or older, and inpatients, although the difference in hospitalization and outpatient was not statistically significant. Patients with complications received lower total doses of propofol and fentanyl per weight per hour. Dexmedetomidine use was significantly associated with complications among inpatients (p = 0.015). The duration of the procedure was longer in patients with complications (p = 0.002).</p><p><strong>Conclusion: </strong>Anesthesia-related complications were frequent among ASA Class III patients who underwent combined EGD and colonoscopy under TIVA, particularly cardiovascular and respiratory events. Identification of five preprocedural risk factors supports the need for improved risk stratification and individualized sedation planning to optimize safety in this high-risk group.</p>\",\"PeriodicalId\":22977,\"journal\":{\"name\":\"Therapeutics and Clinical Risk Management\",\"volume\":\"21 \",\"pages\":\"1395-1408\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-09-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12485486/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutics and Clinical Risk Management\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/TCRM.S541750\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"Pharmacology, Toxicology and Pharmaceutics\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics and Clinical Risk Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/TCRM.S541750","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Pharmacology, Toxicology and Pharmaceutics","Score":null,"Total":0}
Incidence of Complications in High-Risk Patients Undergoing Combined Esophagogastroduodenoscopy and Colonoscopy with Total Intravenous Anesthesia: A Prospective Cohort Study.
Objective: To evaluate the incidence, characteristics, and risk factors of complications related to anesthesia complication in ASA Class III patients undergoing combined esophagogastroduodenoscopy (EGD) and colonoscopy under total intravenous anesthesia (TIVA).
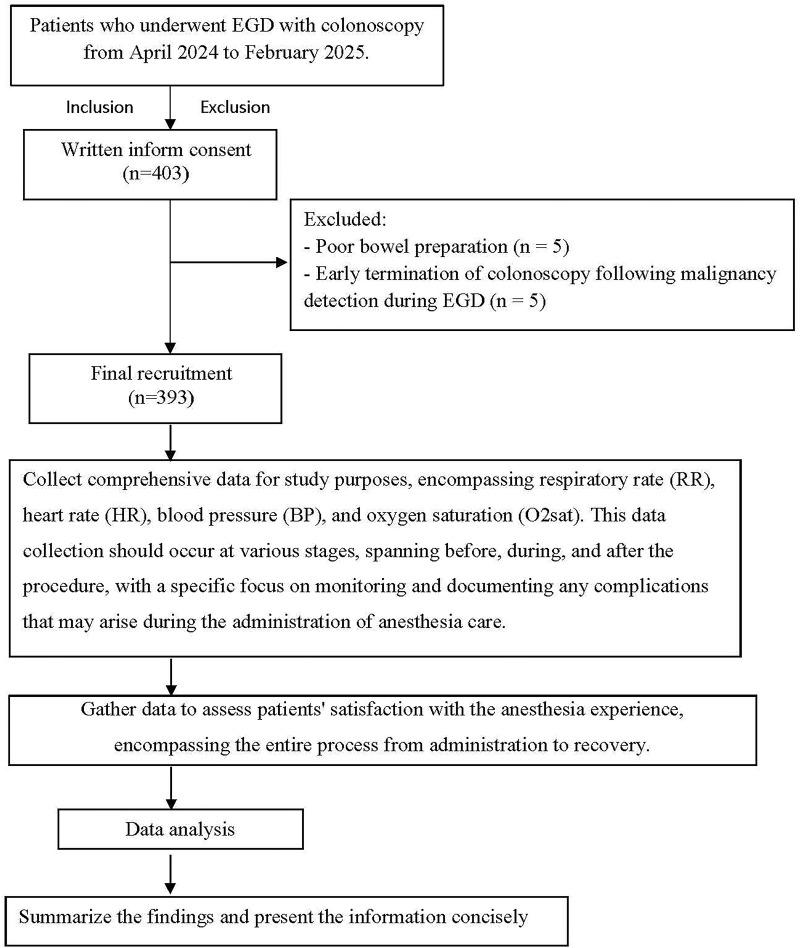
Materials and methods: This prospective cohort study was conducted from April 1, 2024, to February 11, 2025. Data collected included baseline characteristics (age, sex, comorbidities, functional capacity, nutritional status, smoking, fasting and medications) and intraoperative/postoperative parameters (anesthetic technique, sedative dosing, IV fluids, complications, and 24-hour status). Descriptive statistics, univariate analysis, and binary logistic regression were applied.
Results: Of 403 ASA Class III patients enrolled, 393 were analyzed after excluding 10 for inadequate bowel prep or early termination due to malignancy. A total of 207 patients (52.7%) experienced at least one complication. Common complications included transient hypotension (40.2%), desaturation (15.8%), and airway obstruction (15.5%). Less frequent events were bradycardia (4.1%), hypoxia (1.8%), hypertension (1.8%), tachycardia (0.3%) and respiratory depression (0.5%). Five independent risk factors were significantly associated with complications: preexisting cardiovascular disease - odds ratio (OR=1.678), respiratory disease (OR=1.877), functional capacity < 4 metabolic equivalents (METs), (OR=1.851), nutritional screening score ≥1 (OR =1.518), and single - dose bowel prep regimen (OR=1.614). Complications were more common in women, patients aged 65 years or older, and inpatients, although the difference in hospitalization and outpatient was not statistically significant. Patients with complications received lower total doses of propofol and fentanyl per weight per hour. Dexmedetomidine use was significantly associated with complications among inpatients (p = 0.015). The duration of the procedure was longer in patients with complications (p = 0.002).
Conclusion: Anesthesia-related complications were frequent among ASA Class III patients who underwent combined EGD and colonoscopy under TIVA, particularly cardiovascular and respiratory events. Identification of five preprocedural risk factors supports the need for improved risk stratification and individualized sedation planning to optimize safety in this high-risk group.
期刊介绍:
Therapeutics and Clinical Risk Management is an international, peer-reviewed journal of clinical therapeutics and risk management, focusing on concise rapid reporting of clinical studies in all therapeutic areas, outcomes, safety, and programs for the effective, safe, and sustained use of medicines, therapeutic and surgical interventions in all clinical areas.
The journal welcomes submissions covering original research, clinical and epidemiological studies, reviews, guidelines, expert opinion and commentary. The journal will consider case reports but only if they make a valuable and original contribution to the literature.
As of 18th March 2019, Therapeutics and Clinical Risk Management will no longer consider meta-analyses for publication.
The journal does not accept study protocols, animal-based or cell line-based studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


