Aseel AlSaleh, Hebah Abdalla Ali, Amani Ali Almasri, Razan Mahmoud Omoush, Adam Tawfiq Amawi, Mohammed Ahmed Alkharisi, Seithikurippu R Pandi-Perumal, Khaled Trabelsi, Hadeel Ghazzawi, Haitham Jahrami
{"title":"唾液BDNF预测年轻营养学家约旦女性饮食失调的危险状态:来自初步多阶段研究的结果。","authors":"Aseel AlSaleh, Hebah Abdalla Ali, Amani Ali Almasri, Razan Mahmoud Omoush, Adam Tawfiq Amawi, Mohammed Ahmed Alkharisi, Seithikurippu R Pandi-Perumal, Khaled Trabelsi, Hadeel Ghazzawi, Haitham Jahrami","doi":"10.1177/17455057251376885","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Brain-derived neurotrophic factor (BDNF) is associated with the development of different psychiatric conditions, including eating disorders (EDs).</p><p><strong>Objectives: </strong>To investigate the salivary BDNF's ability to act as a potential biomarker for detecting the risk of developing EDs among young females.</p><p><strong>Design and methods: </strong>A cross-sectional study was carried out in Amman, Jordan, with a total of 216 nutrition students completing the Eating Attitudes Test-26 (EAT-26) to assess the risk of developing EDs, the Cohens' Perceived Stress Scale-10 (PSS-10) to measure stress levels, and the International Physical Activity Questionnaire-Short Form (IPAQ-SF) to assess physical activity levels. Dietary intake was analyzed using a semiquantitative food frequency questionnaire. A nested sample of 34 females from both extreme EDs was selected and tested for salivary BDNF levels.</p><p><strong>Results: </strong>The nested sample of 34 female nutrition students 22.00 (2.75) years old with body mass index (BMI) of 23.60 (3.35) kg/m<sup>2</sup> were divided into two groups; 18 students were at lower risk, while 16 were at higher risk of developing EDs. The salivary BDNF levels did not differ significantly between the low-risk and high-risk groups (391.03 (128.17), 339.15 (102.52), and <i>p</i> = 0.347, respectively). BMI, PSS-10 score, and total metabolic equivalent (MET) were significantly different between the two groups. No associations were found between salivary BDNF levels and BMI, PSS-10 score, MET, or different food groups. The odds ratio for the risk of BDNF-related EDs was 1.07 (95% CI, 1.03-1.10) in the higher-risk group versus the lower-risk group.</p><p><strong>Conclusion: </strong>BDNF is not a robust biomarker of risk for EDs. The changes in salivary BDNF levels could reflect individual ED eating patterns rather than indicating a direct causative role in the disorder's development. According to our results, psychiatric consultation for ED detection remains the gold standard for diagnosis and treatment.</p>","PeriodicalId":75327,"journal":{"name":"Women's health (London, England)","volume":"21 ","pages":"17455057251376885"},"PeriodicalIF":2.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12477397/pdf/","citationCount":"0","resultStr":"{\"title\":\"Salivary BDNF to predict at-risk status of eating disorders in young nutritionist Jordanian females: Results from a preliminary multistage study.\",\"authors\":\"Aseel AlSaleh, Hebah Abdalla Ali, Amani Ali Almasri, Razan Mahmoud Omoush, Adam Tawfiq Amawi, Mohammed Ahmed Alkharisi, Seithikurippu R Pandi-Perumal, Khaled Trabelsi, Hadeel Ghazzawi, Haitham Jahrami\",\"doi\":\"10.1177/17455057251376885\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Brain-derived neurotrophic factor (BDNF) is associated with the development of different psychiatric conditions, including eating disorders (EDs).</p><p><strong>Objectives: </strong>To investigate the salivary BDNF's ability to act as a potential biomarker for detecting the risk of developing EDs among young females.</p><p><strong>Design and methods: </strong>A cross-sectional study was carried out in Amman, Jordan, with a total of 216 nutrition students completing the Eating Attitudes Test-26 (EAT-26) to assess the risk of developing EDs, the Cohens' Perceived Stress Scale-10 (PSS-10) to measure stress levels, and the International Physical Activity Questionnaire-Short Form (IPAQ-SF) to assess physical activity levels. Dietary intake was analyzed using a semiquantitative food frequency questionnaire. A nested sample of 34 females from both extreme EDs was selected and tested for salivary BDNF levels.</p><p><strong>Results: </strong>The nested sample of 34 female nutrition students 22.00 (2.75) years old with body mass index (BMI) of 23.60 (3.35) kg/m<sup>2</sup> were divided into two groups; 18 students were at lower risk, while 16 were at higher risk of developing EDs. The salivary BDNF levels did not differ significantly between the low-risk and high-risk groups (391.03 (128.17), 339.15 (102.52), and <i>p</i> = 0.347, respectively). BMI, PSS-10 score, and total metabolic equivalent (MET) were significantly different between the two groups. No associations were found between salivary BDNF levels and BMI, PSS-10 score, MET, or different food groups. The odds ratio for the risk of BDNF-related EDs was 1.07 (95% CI, 1.03-1.10) in the higher-risk group versus the lower-risk group.</p><p><strong>Conclusion: </strong>BDNF is not a robust biomarker of risk for EDs. The changes in salivary BDNF levels could reflect individual ED eating patterns rather than indicating a direct causative role in the disorder's development. According to our results, psychiatric consultation for ED detection remains the gold standard for diagnosis and treatment.</p>\",\"PeriodicalId\":75327,\"journal\":{\"name\":\"Women's health (London, England)\",\"volume\":\"21 \",\"pages\":\"17455057251376885\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12477397/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Women's health (London, England)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/17455057251376885\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Women's health (London, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17455057251376885","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:脑源性神经营养因子(BDNF)与包括饮食失调(EDs)在内的不同精神疾病的发展有关。目的:研究唾液BDNF作为检测年轻女性发生ed风险的潜在生物标志物的能力。设计与方法:在约旦安曼进行横断面研究,共216名营养专业学生完成饮食态度测试-26 (EAT-26)评估发生EDs的风险,Cohens' Perceived Stress Scale-10 (PSS-10)测量压力水平,国际体育活动问卷- short Form (IPAQ-SF)评估体育活动水平。采用半定量食物频率问卷分析饮食摄入量。选取34名来自两种极端ed的女性作为巢状样本,测试唾液BDNF水平。结果:巢式抽样34名年龄22.00(2.75)岁、体重指数(BMI) 23.60 (3.35) kg/m2的营养学女学生分为两组;18名学生患ed的风险较低,16名学生患ed的风险较高。低危组和高危组唾液BDNF水平差异无统计学意义(分别为391.03 (128.17),339.15 (102.52),p = 0.347)。两组患者BMI、PSS-10评分、总代谢当量(MET)差异有统计学意义。唾液BDNF水平与BMI、PSS-10评分、MET或不同食物组之间没有关联。高风险组与低风险组相比,bdnf相关ed风险的优势比为1.07 (95% CI, 1.03-1.10)。结论:BDNF不是ed风险的可靠生物标志物。唾液BDNF水平的变化可能反映了个体ED的饮食模式,而不是表明这种疾病发展的直接病因。根据我们的研究结果,精神科会诊检测ED仍然是诊断和治疗的金标准。
Salivary BDNF to predict at-risk status of eating disorders in young nutritionist Jordanian females: Results from a preliminary multistage study.
Background: Brain-derived neurotrophic factor (BDNF) is associated with the development of different psychiatric conditions, including eating disorders (EDs).
Objectives: To investigate the salivary BDNF's ability to act as a potential biomarker for detecting the risk of developing EDs among young females.
Design and methods: A cross-sectional study was carried out in Amman, Jordan, with a total of 216 nutrition students completing the Eating Attitudes Test-26 (EAT-26) to assess the risk of developing EDs, the Cohens' Perceived Stress Scale-10 (PSS-10) to measure stress levels, and the International Physical Activity Questionnaire-Short Form (IPAQ-SF) to assess physical activity levels. Dietary intake was analyzed using a semiquantitative food frequency questionnaire. A nested sample of 34 females from both extreme EDs was selected and tested for salivary BDNF levels.
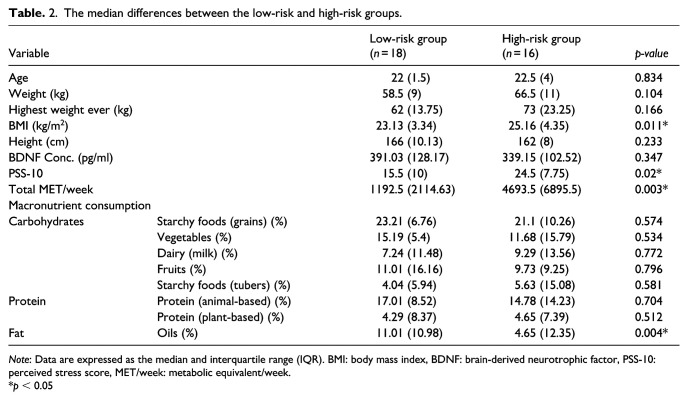
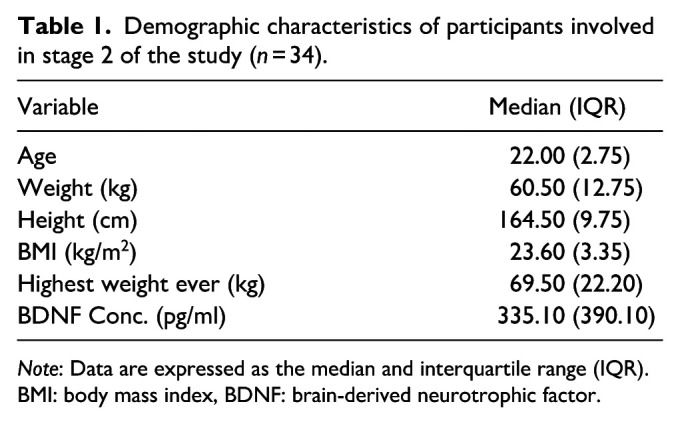
Results: The nested sample of 34 female nutrition students 22.00 (2.75) years old with body mass index (BMI) of 23.60 (3.35) kg/m2 were divided into two groups; 18 students were at lower risk, while 16 were at higher risk of developing EDs. The salivary BDNF levels did not differ significantly between the low-risk and high-risk groups (391.03 (128.17), 339.15 (102.52), and p = 0.347, respectively). BMI, PSS-10 score, and total metabolic equivalent (MET) were significantly different between the two groups. No associations were found between salivary BDNF levels and BMI, PSS-10 score, MET, or different food groups. The odds ratio for the risk of BDNF-related EDs was 1.07 (95% CI, 1.03-1.10) in the higher-risk group versus the lower-risk group.
Conclusion: BDNF is not a robust biomarker of risk for EDs. The changes in salivary BDNF levels could reflect individual ED eating patterns rather than indicating a direct causative role in the disorder's development. According to our results, psychiatric consultation for ED detection remains the gold standard for diagnosis and treatment.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


