Danielle Coombs, Thomas Lung, Marina B Pinheiro, Kirsten Howard, Chris G Maher, Bethan Richards, Chris Needs, Hannah Storey, Gustavo C Machado
{"title":"成本-效果分析的形状试验测试一个多方面的护理模式的实施策略,以改善急诊科护理的腰痛。","authors":"Danielle Coombs, Thomas Lung, Marina B Pinheiro, Kirsten Howard, Chris G Maher, Bethan Richards, Chris Needs, Hannah Storey, Gustavo C Machado","doi":"10.1186/s12962-025-00652-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To test the cost effectiveness of an implementation strategy to promote evidence-based practice for low back pain in the emergency department.</p><p><strong>Methods: </strong>An economic evaluation was conducted alongside a stepped-wedge cluster-randomised controlled trial. The trial aimed to evaluate a strategy to implement a guideline-endorsed model of care in four emergency departments in New South Wales, Australia. The intervention targeted emergency clinicians and was compared to usual emergency care. The main trial outcomes were healthcare use that aligns with the main principles of the model of care. The outcomes explored in this economic evaluation were lumbar imaging referrals, opioid use, and hospital admissions for low back pain. Costs related to implementation development, delivery and healthcare utilisation were included. Bivariate linear multilevel regression analyses were conducted, adjusting for clustering, time and the correlation between cost and outcome to calculate incremental cost and effects and incremental cost-effectiveness ratios. Non-parametric bootstrapping with 5,000 replications of incremental cost and effect pairs was carried out and plotted on cost-effectiveness planes for each of the outcomes. Cost-effectiveness acceptability curves were generated to explore the probability of being cost-effective based on a range of willingness to pay thresholds for each of the outcomes. Sensitivity analyses were carried out to determine to what extent the decision to exclude episodes of care missing healthcare costs and including inpatients costs impacted the results.</p><p><strong>Results: </strong>The implementation was more effective but more costly when considering the three key outcomes. The implementation was cost-effective in reducing opioid use with an incremental cost-effectiveness ratio of $3,574.29 per episode of care where opioids were avoided. The incremental cost effectiveness ratios for avoiding imaging and hospitalisation were $26,298.50 and $49,290.00 per episode of care, respectively. The first sensitivity analysis highlighted uncertainty with the hospital admission result and the second sensitivity analysis found that the implementation was more likely to be cost-effective when considering emergency department costs only.</p><p><strong>Conclusion: </strong>This implementation of the model of care may be cost-effective for reducing opioid use in patients who present to emergency with low back pain, however more research into willingness to pay to avoid opioid use in emergency departments is required.</p>","PeriodicalId":47054,"journal":{"name":"Cost Effectiveness and Resource Allocation","volume":"23 1","pages":"50"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12465644/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-effectiveness analysis of the SHaPED trial testing a multifaceted implementation strategy of a model of care to improve emergency department care of low back pain.\",\"authors\":\"Danielle Coombs, Thomas Lung, Marina B Pinheiro, Kirsten Howard, Chris G Maher, Bethan Richards, Chris Needs, Hannah Storey, Gustavo C Machado\",\"doi\":\"10.1186/s12962-025-00652-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To test the cost effectiveness of an implementation strategy to promote evidence-based practice for low back pain in the emergency department.</p><p><strong>Methods: </strong>An economic evaluation was conducted alongside a stepped-wedge cluster-randomised controlled trial. The trial aimed to evaluate a strategy to implement a guideline-endorsed model of care in four emergency departments in New South Wales, Australia. The intervention targeted emergency clinicians and was compared to usual emergency care. The main trial outcomes were healthcare use that aligns with the main principles of the model of care. The outcomes explored in this economic evaluation were lumbar imaging referrals, opioid use, and hospital admissions for low back pain. Costs related to implementation development, delivery and healthcare utilisation were included. Bivariate linear multilevel regression analyses were conducted, adjusting for clustering, time and the correlation between cost and outcome to calculate incremental cost and effects and incremental cost-effectiveness ratios. Non-parametric bootstrapping with 5,000 replications of incremental cost and effect pairs was carried out and plotted on cost-effectiveness planes for each of the outcomes. Cost-effectiveness acceptability curves were generated to explore the probability of being cost-effective based on a range of willingness to pay thresholds for each of the outcomes. Sensitivity analyses were carried out to determine to what extent the decision to exclude episodes of care missing healthcare costs and including inpatients costs impacted the results.</p><p><strong>Results: </strong>The implementation was more effective but more costly when considering the three key outcomes. The implementation was cost-effective in reducing opioid use with an incremental cost-effectiveness ratio of $3,574.29 per episode of care where opioids were avoided. The incremental cost effectiveness ratios for avoiding imaging and hospitalisation were $26,298.50 and $49,290.00 per episode of care, respectively. The first sensitivity analysis highlighted uncertainty with the hospital admission result and the second sensitivity analysis found that the implementation was more likely to be cost-effective when considering emergency department costs only.</p><p><strong>Conclusion: </strong>This implementation of the model of care may be cost-effective for reducing opioid use in patients who present to emergency with low back pain, however more research into willingness to pay to avoid opioid use in emergency departments is required.</p>\",\"PeriodicalId\":47054,\"journal\":{\"name\":\"Cost Effectiveness and Resource Allocation\",\"volume\":\"23 1\",\"pages\":\"50\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-09-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12465644/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cost Effectiveness and Resource Allocation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12962-025-00652-6\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cost Effectiveness and Resource Allocation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12962-025-00652-6","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
Cost-effectiveness analysis of the SHaPED trial testing a multifaceted implementation strategy of a model of care to improve emergency department care of low back pain.
Objective: To test the cost effectiveness of an implementation strategy to promote evidence-based practice for low back pain in the emergency department.
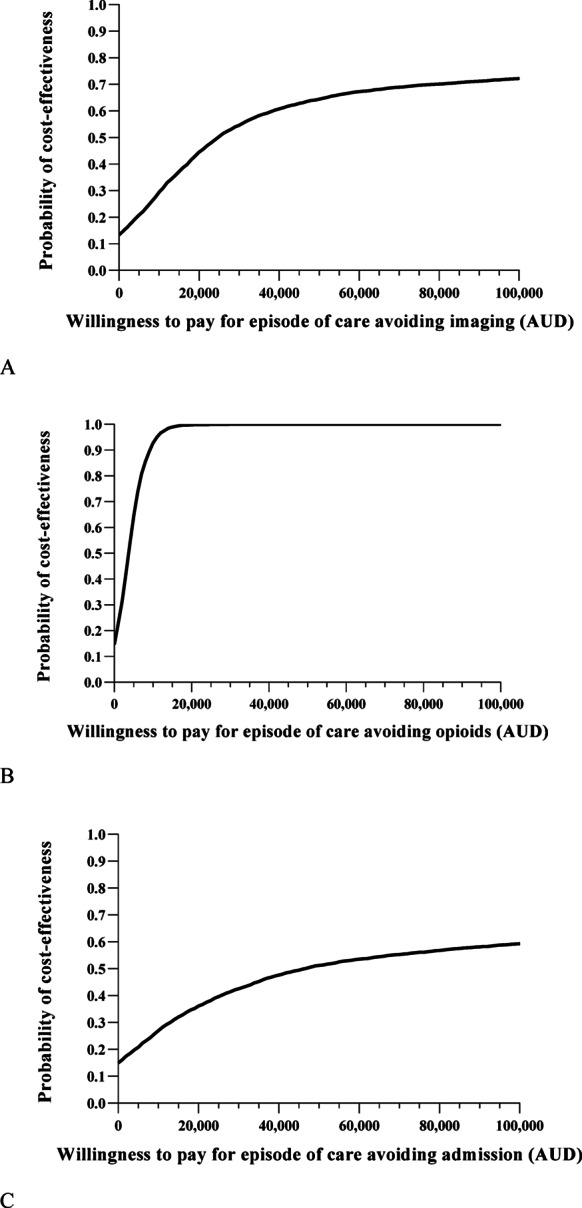
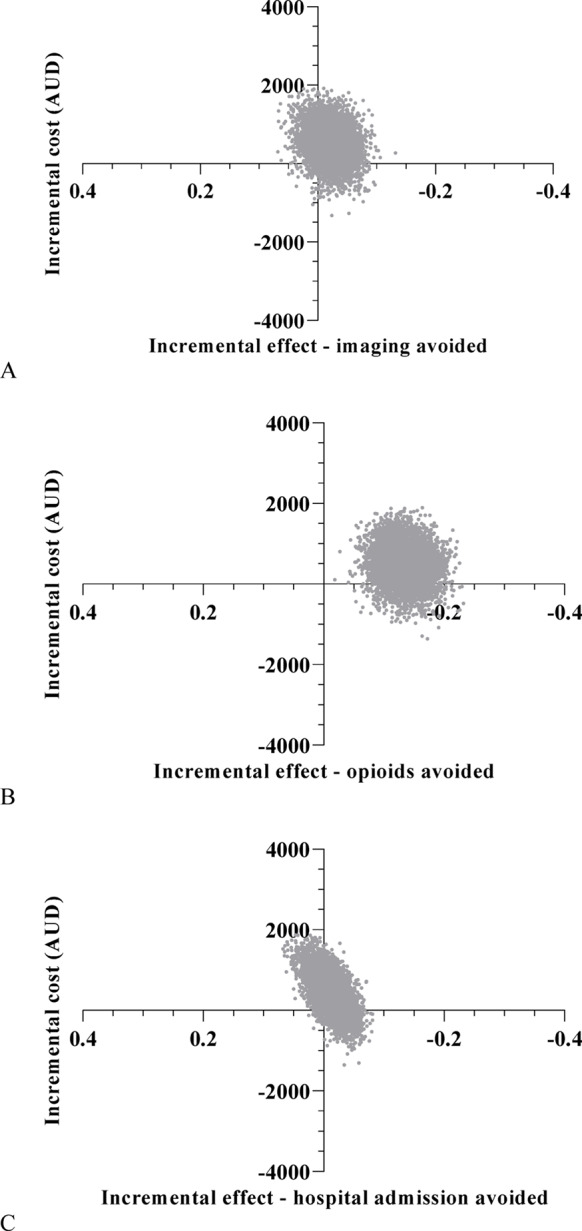
Methods: An economic evaluation was conducted alongside a stepped-wedge cluster-randomised controlled trial. The trial aimed to evaluate a strategy to implement a guideline-endorsed model of care in four emergency departments in New South Wales, Australia. The intervention targeted emergency clinicians and was compared to usual emergency care. The main trial outcomes were healthcare use that aligns with the main principles of the model of care. The outcomes explored in this economic evaluation were lumbar imaging referrals, opioid use, and hospital admissions for low back pain. Costs related to implementation development, delivery and healthcare utilisation were included. Bivariate linear multilevel regression analyses were conducted, adjusting for clustering, time and the correlation between cost and outcome to calculate incremental cost and effects and incremental cost-effectiveness ratios. Non-parametric bootstrapping with 5,000 replications of incremental cost and effect pairs was carried out and plotted on cost-effectiveness planes for each of the outcomes. Cost-effectiveness acceptability curves were generated to explore the probability of being cost-effective based on a range of willingness to pay thresholds for each of the outcomes. Sensitivity analyses were carried out to determine to what extent the decision to exclude episodes of care missing healthcare costs and including inpatients costs impacted the results.
Results: The implementation was more effective but more costly when considering the three key outcomes. The implementation was cost-effective in reducing opioid use with an incremental cost-effectiveness ratio of $3,574.29 per episode of care where opioids were avoided. The incremental cost effectiveness ratios for avoiding imaging and hospitalisation were $26,298.50 and $49,290.00 per episode of care, respectively. The first sensitivity analysis highlighted uncertainty with the hospital admission result and the second sensitivity analysis found that the implementation was more likely to be cost-effective when considering emergency department costs only.
Conclusion: This implementation of the model of care may be cost-effective for reducing opioid use in patients who present to emergency with low back pain, however more research into willingness to pay to avoid opioid use in emergency departments is required.
期刊介绍:
Cost Effectiveness and Resource Allocation is an Open Access, peer-reviewed, online journal that considers manuscripts on all aspects of cost-effectiveness analysis, including conceptual or methodological work, economic evaluations, and policy analysis related to resource allocation at a national or international level. Cost Effectiveness and Resource Allocation is aimed at health economists, health services researchers, and policy-makers with an interest in enhancing the flow and transfer of knowledge relating to efficiency in the health sector. Manuscripts are encouraged from researchers based in low- and middle-income countries, with a view to increasing the international economic evidence base for health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


