{"title":"肾移植后肾小球疾病(GN)复发的叙述性回顾","authors":"Abbal Koirala, Aditi Singh, Duvuru Geetha","doi":"10.3390/jcm14186686","DOIUrl":null,"url":null,"abstract":"<p><p>Recurrence of the original glomerular disease (GN) poses a significant threat to kidney transplant function and longevity. The probability and severity of this recurrence vary, with C3 glomerulopathy and certain forms of FSGS exhibiting particularly high rates. Kidney transplant GN recurrence risk hinges on the characteristics of the initial GN, recipient/donor genetics, recipient age, donor type, end-stage kidney disease (ESRD) progression rate, and proteinuria levels. Standard immunosuppression has limited efficacy in preventing primary disease recurrence; however, agent selection and induction therapy can influence the risk for specific GNs. Diagnosing recurrent GN involves a comprehensive approach, including clinical evaluation, laboratory tests (such as proteinuria, hematuria, and specific biomarkers like anti-PLA2R for membranous nephropathy or complement for C3G), and, critically, an allograft biopsy analyzed with light, immunofluorescence, and electron microscopy. Treatment strategies are evolving towards targeted therapies, such as rituximab for antibody-mediated GN and complement inhibitors for C3G, moving away from broad immunosuppression. This narrative literature review provides practical monitoring algorithms for post-transplant settings, synthesizing information on the incidence, predictors, diagnostic strategies, and therapeutic options for various glomerular disease subtypes. The methodology involved searching MEDLINE, Embase, and Cochrane databases from 1996 to 2025, prioritizing systematic reviews, cohort studies, registries, and interventional reports. Eligibility criteria included adult transplant recipients and English-language reports on recurrent glomerular disease outcomes, excluding most single-patient case reports. Limitations include potential selection bias, omission of relevant studies, and the absence of a formal risk-of-bias assessment or meta-analysis. The evidence base is heterogeneous, with inconsistent outcome reporting and scarce randomized controlled trials. Future efforts should focus on developing predictive biomarkers, standardizing diagnostic and response criteria, conducting multicenter prospective cohorts and pragmatic trials, and creating shared registries with harmonized data.</p>","PeriodicalId":15533,"journal":{"name":"Journal of Clinical Medicine","volume":"14 18","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2025-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12471057/pdf/","citationCount":"0","resultStr":"{\"title\":\"Recurrence of Glomerular Diseases (GN) After Kidney Transplantation: A Narrative Review.\",\"authors\":\"Abbal Koirala, Aditi Singh, Duvuru Geetha\",\"doi\":\"10.3390/jcm14186686\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Recurrence of the original glomerular disease (GN) poses a significant threat to kidney transplant function and longevity. The probability and severity of this recurrence vary, with C3 glomerulopathy and certain forms of FSGS exhibiting particularly high rates. Kidney transplant GN recurrence risk hinges on the characteristics of the initial GN, recipient/donor genetics, recipient age, donor type, end-stage kidney disease (ESRD) progression rate, and proteinuria levels. Standard immunosuppression has limited efficacy in preventing primary disease recurrence; however, agent selection and induction therapy can influence the risk for specific GNs. Diagnosing recurrent GN involves a comprehensive approach, including clinical evaluation, laboratory tests (such as proteinuria, hematuria, and specific biomarkers like anti-PLA2R for membranous nephropathy or complement for C3G), and, critically, an allograft biopsy analyzed with light, immunofluorescence, and electron microscopy. Treatment strategies are evolving towards targeted therapies, such as rituximab for antibody-mediated GN and complement inhibitors for C3G, moving away from broad immunosuppression. This narrative literature review provides practical monitoring algorithms for post-transplant settings, synthesizing information on the incidence, predictors, diagnostic strategies, and therapeutic options for various glomerular disease subtypes. The methodology involved searching MEDLINE, Embase, and Cochrane databases from 1996 to 2025, prioritizing systematic reviews, cohort studies, registries, and interventional reports. Eligibility criteria included adult transplant recipients and English-language reports on recurrent glomerular disease outcomes, excluding most single-patient case reports. Limitations include potential selection bias, omission of relevant studies, and the absence of a formal risk-of-bias assessment or meta-analysis. The evidence base is heterogeneous, with inconsistent outcome reporting and scarce randomized controlled trials. Future efforts should focus on developing predictive biomarkers, standardizing diagnostic and response criteria, conducting multicenter prospective cohorts and pragmatic trials, and creating shared registries with harmonized data.</p>\",\"PeriodicalId\":15533,\"journal\":{\"name\":\"Journal of Clinical Medicine\",\"volume\":\"14 18\",\"pages\":\"\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-09-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12471057/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/jcm14186686\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcm14186686","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Recurrence of Glomerular Diseases (GN) After Kidney Transplantation: A Narrative Review.
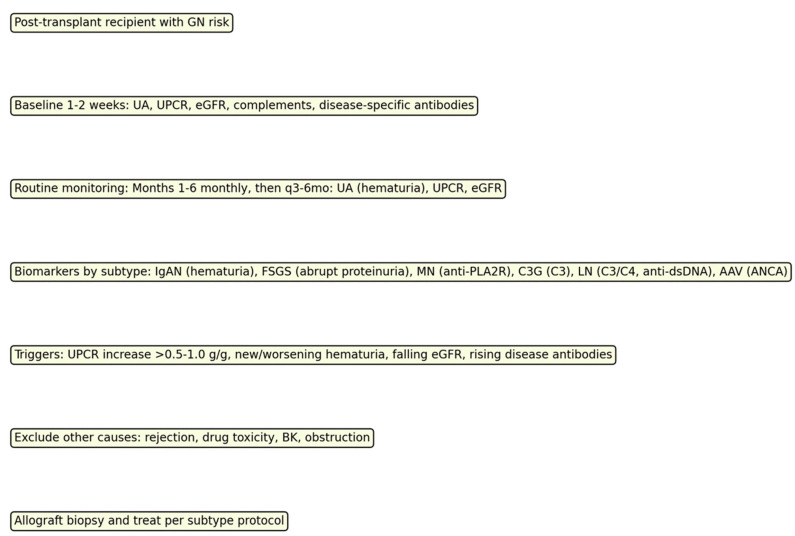
Recurrence of the original glomerular disease (GN) poses a significant threat to kidney transplant function and longevity. The probability and severity of this recurrence vary, with C3 glomerulopathy and certain forms of FSGS exhibiting particularly high rates. Kidney transplant GN recurrence risk hinges on the characteristics of the initial GN, recipient/donor genetics, recipient age, donor type, end-stage kidney disease (ESRD) progression rate, and proteinuria levels. Standard immunosuppression has limited efficacy in preventing primary disease recurrence; however, agent selection and induction therapy can influence the risk for specific GNs. Diagnosing recurrent GN involves a comprehensive approach, including clinical evaluation, laboratory tests (such as proteinuria, hematuria, and specific biomarkers like anti-PLA2R for membranous nephropathy or complement for C3G), and, critically, an allograft biopsy analyzed with light, immunofluorescence, and electron microscopy. Treatment strategies are evolving towards targeted therapies, such as rituximab for antibody-mediated GN and complement inhibitors for C3G, moving away from broad immunosuppression. This narrative literature review provides practical monitoring algorithms for post-transplant settings, synthesizing information on the incidence, predictors, diagnostic strategies, and therapeutic options for various glomerular disease subtypes. The methodology involved searching MEDLINE, Embase, and Cochrane databases from 1996 to 2025, prioritizing systematic reviews, cohort studies, registries, and interventional reports. Eligibility criteria included adult transplant recipients and English-language reports on recurrent glomerular disease outcomes, excluding most single-patient case reports. Limitations include potential selection bias, omission of relevant studies, and the absence of a formal risk-of-bias assessment or meta-analysis. The evidence base is heterogeneous, with inconsistent outcome reporting and scarce randomized controlled trials. Future efforts should focus on developing predictive biomarkers, standardizing diagnostic and response criteria, conducting multicenter prospective cohorts and pragmatic trials, and creating shared registries with harmonized data.
期刊介绍:
Journal of Clinical Medicine (ISSN 2077-0383), is an international scientific open access journal, providing a platform for advances in health care/clinical practices, the study of direct observation of patients and general medical research. This multi-disciplinary journal is aimed at a wide audience of medical researchers and healthcare professionals.
Unique features of this journal:
manuscripts regarding original research and ideas will be particularly welcomed.JCM also accepts reviews, communications, and short notes.
There is no limit to publication length: our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


