{"title":"急性胰腺炎及其并发症的介入治疗。","authors":"Muaaz Masood, Amar Vedamurthy, Rajesh Krishnamoorthi, Shayan Irani, Mehran Fotoohi, Richard Kozarek","doi":"10.3390/jcm14186683","DOIUrl":null,"url":null,"abstract":"<p><p>Acute pancreatitis (AP) is the most common cause of gastrointestinal-related hospitalizations in the United States, with gallstone disease and alcohol as the leading etiologies. Management is determined by disease severity, classified as interstitial edematous pancreatitis or necrotizing pancreatitis, with severity further stratified based on local complications and systemic organ dysfunction. Regardless of etiology, initial treatment involves aggressive intravenous fluid resuscitation with Lactated Ringer's solution, pain and nausea control, early oral feeding in 24 to 48 h, and etiology-directed interventions when indicated. In gallstone pancreatitis, early endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy is indicated in the presence of concomitant cholangitis or persistent biliary obstruction, with subsequent laparoscopic cholecystectomy as standard of care for stone clearance. The role of interventional therapy in uncomplicated AP is limited in the acute phase, except for biliary decompression or enteral feeding support with nasojejunal tube placement. However, in severe AP with complications, interventional radiology (IR) and endoscopic approaches play a pivotal role. IR facilitates early percutaneous drainage of symptomatic, acute fluid collections and infected necrosis, particularly in non-endoscopically accessible retroperitoneal or dependent collections, improving outcomes with a step-up approach. IR-guided angiographic embolization is the preferred modality for hemorrhagic complications, including pseudoaneurysms. In the delayed phase, walled-off necrosis (WON) and pancreatic pseudocysts are managed with endoscopic ultrasound (EUS)-guided drainage, with direct endoscopic necrosectomy (DEN) reserved for infected necrosis. Dual-modality drainage (DMD), combining percutaneous and endoscopic drainage, is increasingly utilized in extensive or complex collections, reflecting a collaborative effort between gastroenterology and interventional radiology comparable to that which exists between IR and surgery in institutions that perform video assisted retroperitoneal debridement (VARD). Peripancreatic fluid collections may fistulize into adjacent structures, including the stomach, small intestine, or colon, requiring transpapillary stenting with or without additional closure of the gut leak with over-the-scope clips (OTSC) or suturing devices. Additionally, endoscopic management of pancreatic duct disruptions with transpapillary or transmural stenting plays a key role in cases of disconnected pancreatic duct syndrome (DPDS). Comparative outcomes across interventional techniques-including retroperitoneal, laparoscopic, open surgery, and endoscopic drainage-highlight a shift toward minimally invasive approaches, with decreased morbidity and reduced hospital stay. The integration of endoscopic and interventional radiology-guided techniques has transformed the management of AP complications and multidisciplinary collaboration is essential for optimal patient outcomes.</p>","PeriodicalId":15533,"journal":{"name":"Journal of Clinical Medicine","volume":"14 18","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2025-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12470711/pdf/","citationCount":"0","resultStr":"{\"title\":\"Interventional Management of Acute Pancreatitis and Its Complications.\",\"authors\":\"Muaaz Masood, Amar Vedamurthy, Rajesh Krishnamoorthi, Shayan Irani, Mehran Fotoohi, Richard Kozarek\",\"doi\":\"10.3390/jcm14186683\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Acute pancreatitis (AP) is the most common cause of gastrointestinal-related hospitalizations in the United States, with gallstone disease and alcohol as the leading etiologies. Management is determined by disease severity, classified as interstitial edematous pancreatitis or necrotizing pancreatitis, with severity further stratified based on local complications and systemic organ dysfunction. Regardless of etiology, initial treatment involves aggressive intravenous fluid resuscitation with Lactated Ringer's solution, pain and nausea control, early oral feeding in 24 to 48 h, and etiology-directed interventions when indicated. In gallstone pancreatitis, early endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy is indicated in the presence of concomitant cholangitis or persistent biliary obstruction, with subsequent laparoscopic cholecystectomy as standard of care for stone clearance. The role of interventional therapy in uncomplicated AP is limited in the acute phase, except for biliary decompression or enteral feeding support with nasojejunal tube placement. However, in severe AP with complications, interventional radiology (IR) and endoscopic approaches play a pivotal role. IR facilitates early percutaneous drainage of symptomatic, acute fluid collections and infected necrosis, particularly in non-endoscopically accessible retroperitoneal or dependent collections, improving outcomes with a step-up approach. IR-guided angiographic embolization is the preferred modality for hemorrhagic complications, including pseudoaneurysms. In the delayed phase, walled-off necrosis (WON) and pancreatic pseudocysts are managed with endoscopic ultrasound (EUS)-guided drainage, with direct endoscopic necrosectomy (DEN) reserved for infected necrosis. Dual-modality drainage (DMD), combining percutaneous and endoscopic drainage, is increasingly utilized in extensive or complex collections, reflecting a collaborative effort between gastroenterology and interventional radiology comparable to that which exists between IR and surgery in institutions that perform video assisted retroperitoneal debridement (VARD). Peripancreatic fluid collections may fistulize into adjacent structures, including the stomach, small intestine, or colon, requiring transpapillary stenting with or without additional closure of the gut leak with over-the-scope clips (OTSC) or suturing devices. Additionally, endoscopic management of pancreatic duct disruptions with transpapillary or transmural stenting plays a key role in cases of disconnected pancreatic duct syndrome (DPDS). Comparative outcomes across interventional techniques-including retroperitoneal, laparoscopic, open surgery, and endoscopic drainage-highlight a shift toward minimally invasive approaches, with decreased morbidity and reduced hospital stay. The integration of endoscopic and interventional radiology-guided techniques has transformed the management of AP complications and multidisciplinary collaboration is essential for optimal patient outcomes.</p>\",\"PeriodicalId\":15533,\"journal\":{\"name\":\"Journal of Clinical Medicine\",\"volume\":\"14 18\",\"pages\":\"\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-09-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12470711/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/jcm14186683\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcm14186683","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Interventional Management of Acute Pancreatitis and Its Complications.
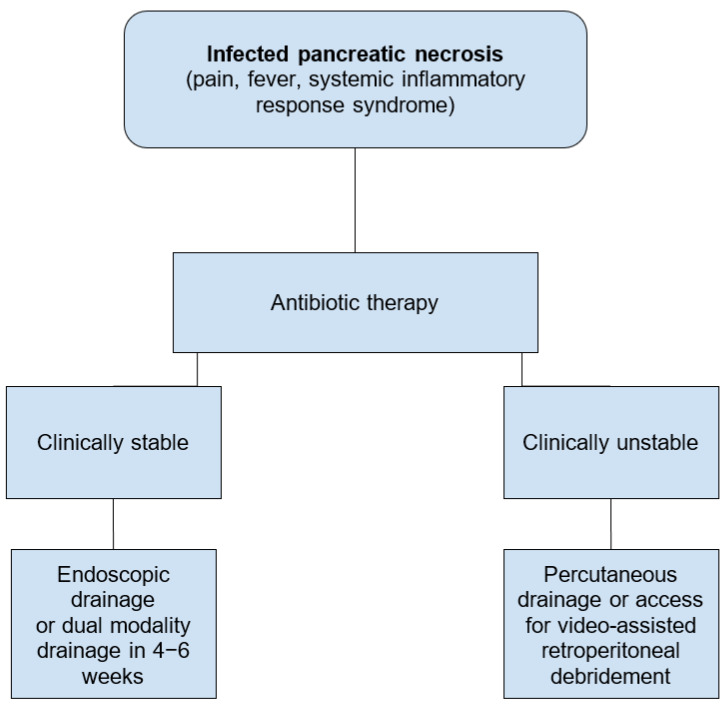
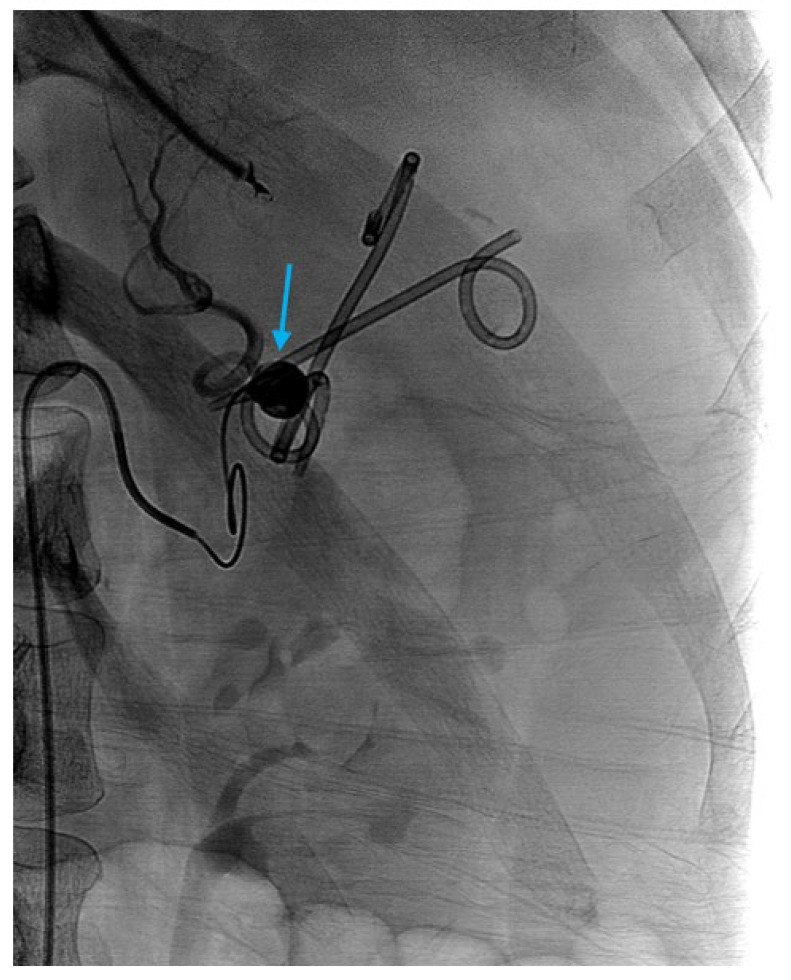
Acute pancreatitis (AP) is the most common cause of gastrointestinal-related hospitalizations in the United States, with gallstone disease and alcohol as the leading etiologies. Management is determined by disease severity, classified as interstitial edematous pancreatitis or necrotizing pancreatitis, with severity further stratified based on local complications and systemic organ dysfunction. Regardless of etiology, initial treatment involves aggressive intravenous fluid resuscitation with Lactated Ringer's solution, pain and nausea control, early oral feeding in 24 to 48 h, and etiology-directed interventions when indicated. In gallstone pancreatitis, early endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy is indicated in the presence of concomitant cholangitis or persistent biliary obstruction, with subsequent laparoscopic cholecystectomy as standard of care for stone clearance. The role of interventional therapy in uncomplicated AP is limited in the acute phase, except for biliary decompression or enteral feeding support with nasojejunal tube placement. However, in severe AP with complications, interventional radiology (IR) and endoscopic approaches play a pivotal role. IR facilitates early percutaneous drainage of symptomatic, acute fluid collections and infected necrosis, particularly in non-endoscopically accessible retroperitoneal or dependent collections, improving outcomes with a step-up approach. IR-guided angiographic embolization is the preferred modality for hemorrhagic complications, including pseudoaneurysms. In the delayed phase, walled-off necrosis (WON) and pancreatic pseudocysts are managed with endoscopic ultrasound (EUS)-guided drainage, with direct endoscopic necrosectomy (DEN) reserved for infected necrosis. Dual-modality drainage (DMD), combining percutaneous and endoscopic drainage, is increasingly utilized in extensive or complex collections, reflecting a collaborative effort between gastroenterology and interventional radiology comparable to that which exists between IR and surgery in institutions that perform video assisted retroperitoneal debridement (VARD). Peripancreatic fluid collections may fistulize into adjacent structures, including the stomach, small intestine, or colon, requiring transpapillary stenting with or without additional closure of the gut leak with over-the-scope clips (OTSC) or suturing devices. Additionally, endoscopic management of pancreatic duct disruptions with transpapillary or transmural stenting plays a key role in cases of disconnected pancreatic duct syndrome (DPDS). Comparative outcomes across interventional techniques-including retroperitoneal, laparoscopic, open surgery, and endoscopic drainage-highlight a shift toward minimally invasive approaches, with decreased morbidity and reduced hospital stay. The integration of endoscopic and interventional radiology-guided techniques has transformed the management of AP complications and multidisciplinary collaboration is essential for optimal patient outcomes.
期刊介绍:
Journal of Clinical Medicine (ISSN 2077-0383), is an international scientific open access journal, providing a platform for advances in health care/clinical practices, the study of direct observation of patients and general medical research. This multi-disciplinary journal is aimed at a wide audience of medical researchers and healthcare professionals.
Unique features of this journal:
manuscripts regarding original research and ideas will be particularly welcomed.JCM also accepts reviews, communications, and short notes.
There is no limit to publication length: our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


