JooYoung Lee, JaeHwan Cho, Dong-Ho Lee, ChangJu Hwang, SeHan Park
{"title":"融合术后上邻节段早期变化的影像学分析:OLIF与PLIF。","authors":"JooYoung Lee, JaeHwan Cho, Dong-Ho Lee, ChangJu Hwang, SeHan Park","doi":"10.3390/jcm14186570","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Oblique lumbar interbody fusion (OLIF) has recently gained popularity as a minimally invasive surgical technique for lumbar fusion. While OLIF is superior in restoring disc height and lumbar lordosis compared to posterior lumbar interbody fusion (PLIF), its biomechanical effect on adjacent segments remains unclear. <b>Methods:</b> We retrospectively analyzed 236 patients who underwent one- or two-level OLIF (<i>n</i> = 95) or PLIF (<i>n</i> = 141) between 2013 and 2020. Radiographic outcomes, including lumbar lordosis, upper adjacent segmental lordosis, retrolisthesis, and foraminal height, were evaluated preoperatively and at 3 days and 1, 3, 6, and 12 months postoperatively. Patient-reported outcomes (VAS for back/leg pain and Oswestry Disability Index [ODI]) were assessed preoperatively and at 12 months. <b>Results:</b> OLIF provided superior restoration of lumbar lordosis (4.03 ± 4.38° vs. 1.63 ± 5.11°, <i>p</i> = 0.001) and disc height (5.50 ± 3.39 mm vs. 2.71 ± 2.18 mm, <i>p</i> < 0.0001) compared with PLIF. However, OLIF was associated with higher incidence (76.9% vs. 24.6%, <i>p</i> < 0.0001) and degree of retrolisthesis (1.69 ± 1.09 mm vs. 0.29 ± 0.70 mm, <i>p</i> < 0.0001), and decreased foraminal height (-1.43 ± 2.12 mm vs. 0.54 ± 2.53 mm, <i>p</i> < 0.0001) in the upper adjacent segment. Importantly, there was no significant difference in clinical outcomes (VAS and ODI) between the two groups at 12 months (all <i>p</i> > 0.05). <b>Conclusions:</b> While OLIF achieves superior restoration of lumbar lordosis and disc height compared to PLIF, it also induces early radiographic deterioration in the upper adjacent segment. Importantly, these findings represent radiographic changes observed within 1 year, without significant differences in clinical outcomes, and longer-term follow-up is required to determine their clinical relevance.</p>","PeriodicalId":15533,"journal":{"name":"Journal of Clinical Medicine","volume":"14 18","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2025-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12471009/pdf/","citationCount":"0","resultStr":"{\"title\":\"Radiographic Analysis of Early Changes in Upper Adjacent Segments After Fusion Surgery: OLIF vs. PLIF.\",\"authors\":\"JooYoung Lee, JaeHwan Cho, Dong-Ho Lee, ChangJu Hwang, SeHan Park\",\"doi\":\"10.3390/jcm14186570\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Oblique lumbar interbody fusion (OLIF) has recently gained popularity as a minimally invasive surgical technique for lumbar fusion. While OLIF is superior in restoring disc height and lumbar lordosis compared to posterior lumbar interbody fusion (PLIF), its biomechanical effect on adjacent segments remains unclear. <b>Methods:</b> We retrospectively analyzed 236 patients who underwent one- or two-level OLIF (<i>n</i> = 95) or PLIF (<i>n</i> = 141) between 2013 and 2020. Radiographic outcomes, including lumbar lordosis, upper adjacent segmental lordosis, retrolisthesis, and foraminal height, were evaluated preoperatively and at 3 days and 1, 3, 6, and 12 months postoperatively. Patient-reported outcomes (VAS for back/leg pain and Oswestry Disability Index [ODI]) were assessed preoperatively and at 12 months. <b>Results:</b> OLIF provided superior restoration of lumbar lordosis (4.03 ± 4.38° vs. 1.63 ± 5.11°, <i>p</i> = 0.001) and disc height (5.50 ± 3.39 mm vs. 2.71 ± 2.18 mm, <i>p</i> < 0.0001) compared with PLIF. However, OLIF was associated with higher incidence (76.9% vs. 24.6%, <i>p</i> < 0.0001) and degree of retrolisthesis (1.69 ± 1.09 mm vs. 0.29 ± 0.70 mm, <i>p</i> < 0.0001), and decreased foraminal height (-1.43 ± 2.12 mm vs. 0.54 ± 2.53 mm, <i>p</i> < 0.0001) in the upper adjacent segment. Importantly, there was no significant difference in clinical outcomes (VAS and ODI) between the two groups at 12 months (all <i>p</i> > 0.05). <b>Conclusions:</b> While OLIF achieves superior restoration of lumbar lordosis and disc height compared to PLIF, it also induces early radiographic deterioration in the upper adjacent segment. Importantly, these findings represent radiographic changes observed within 1 year, without significant differences in clinical outcomes, and longer-term follow-up is required to determine their clinical relevance.</p>\",\"PeriodicalId\":15533,\"journal\":{\"name\":\"Journal of Clinical Medicine\",\"volume\":\"14 18\",\"pages\":\"\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12471009/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/jcm14186570\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcm14186570","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
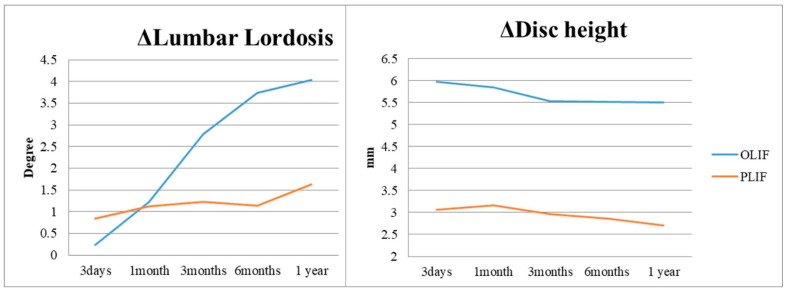
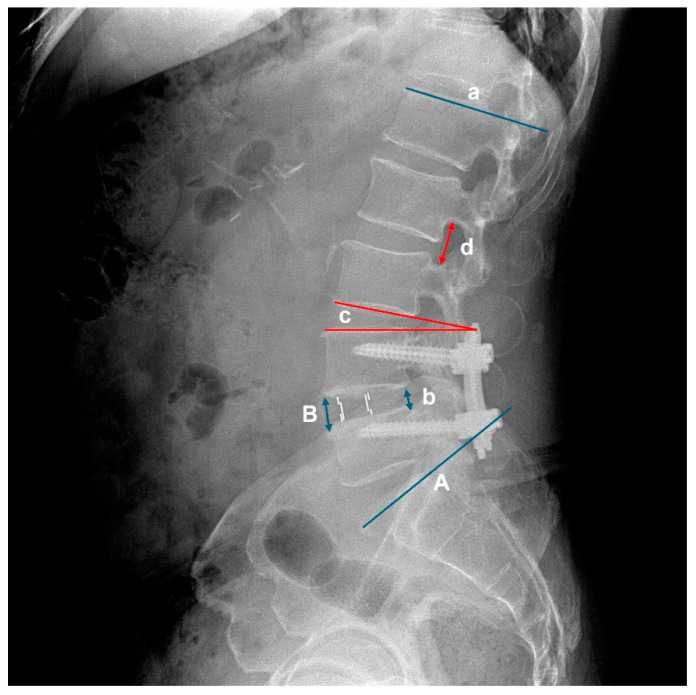
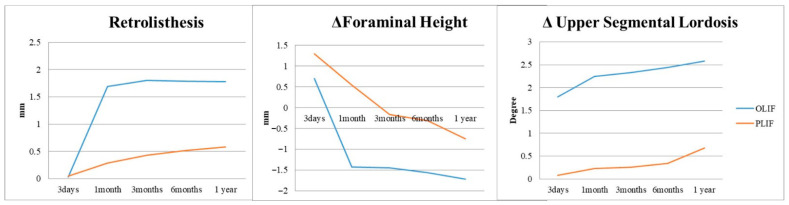
背景:斜腰椎椎体间融合术(OLIF)最近作为一种微创腰椎融合术得到了广泛的应用。虽然OLIF在恢复椎间盘高度和腰椎前凸方面优于后路腰椎椎体间融合术(PLIF),但其对邻近节段的生物力学影响尚不清楚。方法:我们回顾性分析了2013年至2020年间接受一级或二级OLIF (n = 95)或PLIF (n = 141)的236例患者。术前、术后3天、1、3、6、12个月评估影像学结果,包括腰椎前凸、上相邻节段前凸、后滑脱和椎间孔高度。术前和12个月时评估患者报告的结果(背部/腿部疼痛的VAS评分和Oswestry残疾指数[ODI])。结果:OLIF在腰椎前凸(4.03±4.38°vs. 1.63±5.11°,p = 0.001)和椎间盘高度(5.50±3.39 mm vs. 2.71±2.18 mm, p < 0.0001)方面优于PLIF。然而,OLIF与较高的发病率(76.9% vs. 24.6%, p < 0.0001)、后滑脱程度(1.69±1.09 mm vs. 0.29±0.70 mm, p < 0.0001)以及上相邻节段椎间孔高度降低(-1.43±2.12 mm vs. 0.54±2.53 mm, p < 0.0001)相关。重要的是,两组在12个月时的临床结果(VAS和ODI)无显著差异(均p < 0.05)。结论:与PLIF相比,OLIF可以更好地恢复腰椎前凸和椎间盘高度,但它也会导致上邻近节段早期影像学恶化。重要的是,这些发现代表了1年内观察到的影像学变化,临床结果无显著差异,需要长期随访以确定其临床相关性。
Radiographic Analysis of Early Changes in Upper Adjacent Segments After Fusion Surgery: OLIF vs. PLIF.
Background: Oblique lumbar interbody fusion (OLIF) has recently gained popularity as a minimally invasive surgical technique for lumbar fusion. While OLIF is superior in restoring disc height and lumbar lordosis compared to posterior lumbar interbody fusion (PLIF), its biomechanical effect on adjacent segments remains unclear. Methods: We retrospectively analyzed 236 patients who underwent one- or two-level OLIF (n = 95) or PLIF (n = 141) between 2013 and 2020. Radiographic outcomes, including lumbar lordosis, upper adjacent segmental lordosis, retrolisthesis, and foraminal height, were evaluated preoperatively and at 3 days and 1, 3, 6, and 12 months postoperatively. Patient-reported outcomes (VAS for back/leg pain and Oswestry Disability Index [ODI]) were assessed preoperatively and at 12 months. Results: OLIF provided superior restoration of lumbar lordosis (4.03 ± 4.38° vs. 1.63 ± 5.11°, p = 0.001) and disc height (5.50 ± 3.39 mm vs. 2.71 ± 2.18 mm, p < 0.0001) compared with PLIF. However, OLIF was associated with higher incidence (76.9% vs. 24.6%, p < 0.0001) and degree of retrolisthesis (1.69 ± 1.09 mm vs. 0.29 ± 0.70 mm, p < 0.0001), and decreased foraminal height (-1.43 ± 2.12 mm vs. 0.54 ± 2.53 mm, p < 0.0001) in the upper adjacent segment. Importantly, there was no significant difference in clinical outcomes (VAS and ODI) between the two groups at 12 months (all p > 0.05). Conclusions: While OLIF achieves superior restoration of lumbar lordosis and disc height compared to PLIF, it also induces early radiographic deterioration in the upper adjacent segment. Importantly, these findings represent radiographic changes observed within 1 year, without significant differences in clinical outcomes, and longer-term follow-up is required to determine their clinical relevance.
期刊介绍:
Journal of Clinical Medicine (ISSN 2077-0383), is an international scientific open access journal, providing a platform for advances in health care/clinical practices, the study of direct observation of patients and general medical research. This multi-disciplinary journal is aimed at a wide audience of medical researchers and healthcare professionals.
Unique features of this journal:
manuscripts regarding original research and ideas will be particularly welcomed.JCM also accepts reviews, communications, and short notes.
There is no limit to publication length: our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


