David Maman, Maneesh Nandakumar, Yaniv Steinfeld, Yaron Berkovich
{"title":"术前阿片类药物使用障碍预测ACDF术后通气时间延长、中央静脉导管放置和主要麻醉并发症:18万例大数据分析","authors":"David Maman, Maneesh Nandakumar, Yaniv Steinfeld, Yaron Berkovich","doi":"10.3390/jcm14186661","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Opioid use disorder (OUD) has emerged as a growing public health challenge, increasingly affecting surgical populations. While anterior cervical discectomy and fusion (ACDF) is a common spinal procedure with known perioperative risks, the specific impact of preoperative OUD on anesthesia-related complications in ACDF remains poorly studied. <b>Methods:</b> We analyzed adult patients undergoing elective single-level ACDF between 2016 and 2022 using the Nationwide Inpatient Sample (NIS) database. Patients with and without OUD were identified using ICD-10 codes. Propensity score matching was applied to adjust for baseline differences. Primary outcomes included prolonged ventilation, central line placement, and major anesthesiology complications. Secondary outcomes included total charges, length of stay, and number of procedures. A cost-effectiveness analysis of universal preoperative urine drug screening was also performed. <b>Results:</b> Among 178,215 patients undergoing ACDF, 1.5% had documented OUD. Following propensity matching, OUD patients had a significantly increased risk of prolonged ventilation (>24 h and >96 h), central line placement, blood transfusion, feeding tube insertion, and major anesthesiology complications. OUD patients experienced longer hospital stays (7.9 vs. 2.7 days), more procedures (4.2 vs. 3.0), and higher total charges ($139,207 vs. $82,179; all <i>p</i> < 0.01). The estimated excess cost attributable to OUD per surgical patient was $855, compared to a $75 screening cost. <b>Conclusions:</b> Preoperative OUD is associated with significantly increased perioperative risk, ICU-level intervention, and healthcare costs in ACDF patients. These findings support systematic preoperative screening and multidisciplinary management for patients with OUD undergoing spine surgery.</p>","PeriodicalId":15533,"journal":{"name":"Journal of Clinical Medicine","volume":"14 18","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2025-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12470753/pdf/","citationCount":"0","resultStr":"{\"title\":\"Preoperative Opioid Use Disorder Predicts Prolonged Ventilation, Central Line Placement, and Major Anesthesiology Complications After ACDF Surgery: A Big Data Analysis of 180,000 Cases.\",\"authors\":\"David Maman, Maneesh Nandakumar, Yaniv Steinfeld, Yaron Berkovich\",\"doi\":\"10.3390/jcm14186661\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Opioid use disorder (OUD) has emerged as a growing public health challenge, increasingly affecting surgical populations. While anterior cervical discectomy and fusion (ACDF) is a common spinal procedure with known perioperative risks, the specific impact of preoperative OUD on anesthesia-related complications in ACDF remains poorly studied. <b>Methods:</b> We analyzed adult patients undergoing elective single-level ACDF between 2016 and 2022 using the Nationwide Inpatient Sample (NIS) database. Patients with and without OUD were identified using ICD-10 codes. Propensity score matching was applied to adjust for baseline differences. Primary outcomes included prolonged ventilation, central line placement, and major anesthesiology complications. Secondary outcomes included total charges, length of stay, and number of procedures. A cost-effectiveness analysis of universal preoperative urine drug screening was also performed. <b>Results:</b> Among 178,215 patients undergoing ACDF, 1.5% had documented OUD. Following propensity matching, OUD patients had a significantly increased risk of prolonged ventilation (>24 h and >96 h), central line placement, blood transfusion, feeding tube insertion, and major anesthesiology complications. OUD patients experienced longer hospital stays (7.9 vs. 2.7 days), more procedures (4.2 vs. 3.0), and higher total charges ($139,207 vs. $82,179; all <i>p</i> < 0.01). The estimated excess cost attributable to OUD per surgical patient was $855, compared to a $75 screening cost. <b>Conclusions:</b> Preoperative OUD is associated with significantly increased perioperative risk, ICU-level intervention, and healthcare costs in ACDF patients. These findings support systematic preoperative screening and multidisciplinary management for patients with OUD undergoing spine surgery.</p>\",\"PeriodicalId\":15533,\"journal\":{\"name\":\"Journal of Clinical Medicine\",\"volume\":\"14 18\",\"pages\":\"\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-09-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12470753/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/jcm14186661\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcm14186661","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Preoperative Opioid Use Disorder Predicts Prolonged Ventilation, Central Line Placement, and Major Anesthesiology Complications After ACDF Surgery: A Big Data Analysis of 180,000 Cases.
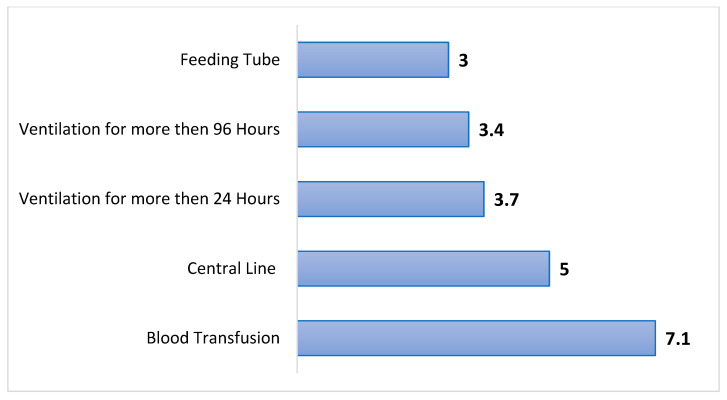
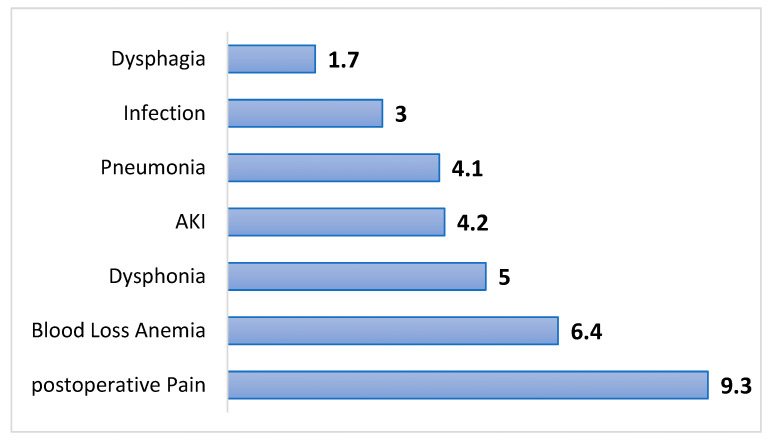
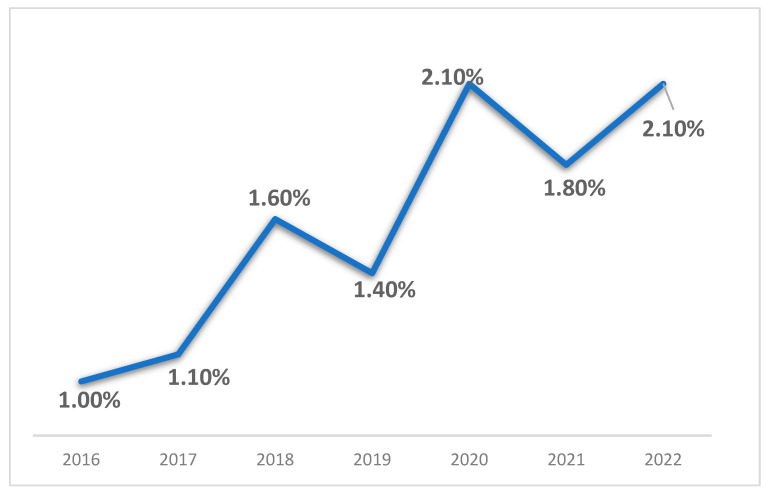
Background: Opioid use disorder (OUD) has emerged as a growing public health challenge, increasingly affecting surgical populations. While anterior cervical discectomy and fusion (ACDF) is a common spinal procedure with known perioperative risks, the specific impact of preoperative OUD on anesthesia-related complications in ACDF remains poorly studied. Methods: We analyzed adult patients undergoing elective single-level ACDF between 2016 and 2022 using the Nationwide Inpatient Sample (NIS) database. Patients with and without OUD were identified using ICD-10 codes. Propensity score matching was applied to adjust for baseline differences. Primary outcomes included prolonged ventilation, central line placement, and major anesthesiology complications. Secondary outcomes included total charges, length of stay, and number of procedures. A cost-effectiveness analysis of universal preoperative urine drug screening was also performed. Results: Among 178,215 patients undergoing ACDF, 1.5% had documented OUD. Following propensity matching, OUD patients had a significantly increased risk of prolonged ventilation (>24 h and >96 h), central line placement, blood transfusion, feeding tube insertion, and major anesthesiology complications. OUD patients experienced longer hospital stays (7.9 vs. 2.7 days), more procedures (4.2 vs. 3.0), and higher total charges ($139,207 vs. $82,179; all p < 0.01). The estimated excess cost attributable to OUD per surgical patient was $855, compared to a $75 screening cost. Conclusions: Preoperative OUD is associated with significantly increased perioperative risk, ICU-level intervention, and healthcare costs in ACDF patients. These findings support systematic preoperative screening and multidisciplinary management for patients with OUD undergoing spine surgery.
期刊介绍:
Journal of Clinical Medicine (ISSN 2077-0383), is an international scientific open access journal, providing a platform for advances in health care/clinical practices, the study of direct observation of patients and general medical research. This multi-disciplinary journal is aimed at a wide audience of medical researchers and healthcare professionals.
Unique features of this journal:
manuscripts regarding original research and ideas will be particularly welcomed.JCM also accepts reviews, communications, and short notes.
There is no limit to publication length: our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


