Umberto Anceschi, Antonio Tufano, Rocco Simone Flammia, Eugenio Bologna, Riccardo Mastroianni, Leslie Claire Licari, Aldo Brassetti, Maria Consiglia Ferriero, Alfredo Maria Bove, Gabriele Tuderti, Simone D'Annunzio, Maddalena Iori, Silvia Cartolano, Marco Pula, Costantino Leonardo, Giuseppe Simone
{"title":"老年患者的手术决策框架:中期随访的I期肾细胞癌的微创部分肾切除术与根治性肾切除术。","authors":"Umberto Anceschi, Antonio Tufano, Rocco Simone Flammia, Eugenio Bologna, Riccardo Mastroianni, Leslie Claire Licari, Aldo Brassetti, Maria Consiglia Ferriero, Alfredo Maria Bove, Gabriele Tuderti, Simone D'Annunzio, Maddalena Iori, Silvia Cartolano, Marco Pula, Costantino Leonardo, Giuseppe Simone","doi":"10.3390/jcm14186634","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background/Objectives</b>: The optimal surgical approach for stage I renal cell carcinoma (RCC) in ultra-octogenarians remains debated, especially when balancing oncologic control, renal preservation, and procedural safety. While ablative techniques and active surveillance are often favored in frail patients, robust comparative evidence supporting nephron-sparing surgery in this age group is limited. <b>Methods</b>: We retrospectively reviewed consecutive patients aged ≥80 years who underwent minimally invasive surgery for cT1 clear cell RCC at a high-volume tertiary-care center between July 2001 and August 2025. Patients were stratified into two cohorts: minimally invasive partial nephrectomy (MIPN, <i>n</i> = 51) and radical nephrectomy (MIRN, n = 26). All MIPNs were performed using an off-clamp approach. Baseline, perioperative, functional, and oncologic outcomes were compared. Kaplan-Meier analysis estimated overall survival (OS), cancer-specific survival (CSS), and progression to significant chronic kidney disease (sCKD, defined as CKD stage ≥ 3b). <b>Results</b>: Groups were comparable in age, comorbidities, and ASA score. MIRN patients exhibited higher tumor complexity (RENAL score: 9 vs. 7, <i>p</i> = 0.01) and a greater proportion of pT1b lesions (77% vs. 37.3%, <i>p</i> = 0.01). Perioperative transfusions occurred exclusively in the MIRN group (<i>p</i> = 0.01), whereas complication rates were low and similar between groups. MIPN was associated with significantly higher eGFR at follow-up (48 vs. 30.9 mL/min/1.73 m<sup>2</sup>, <i>p</i> = 0.01) and a delayed progression to sCKD (<i>p</i> = 0.01), with no differences in OS or CSS at a median follow-up of 30.5 months. <b>Conclusions</b>: In this real-world series of ultra-octogenarians with cT1 clear cell RCC, off-clamp minimally invasive partial nephrectomy ensured superior renal function preservation and delayed progression to sCKD, without compromising oncologic control at mid-term follow-up. Beyond statistical outcomes, these results underscore the importance of tailoring surgical strategies to protect long-term functional autonomy and preserve physiological resilience in elderly patients.</p>","PeriodicalId":15533,"journal":{"name":"Journal of Clinical Medicine","volume":"14 18","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2025-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12471238/pdf/","citationCount":"0","resultStr":"{\"title\":\"Framing Surgical Decisions in Elderly Patients: Minimally Invasive Partial Versus Radical Nephrectomy for Stage I Renal Cell Carcinoma at Mid-Term Follow-Up.\",\"authors\":\"Umberto Anceschi, Antonio Tufano, Rocco Simone Flammia, Eugenio Bologna, Riccardo Mastroianni, Leslie Claire Licari, Aldo Brassetti, Maria Consiglia Ferriero, Alfredo Maria Bove, Gabriele Tuderti, Simone D'Annunzio, Maddalena Iori, Silvia Cartolano, Marco Pula, Costantino Leonardo, Giuseppe Simone\",\"doi\":\"10.3390/jcm14186634\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background/Objectives</b>: The optimal surgical approach for stage I renal cell carcinoma (RCC) in ultra-octogenarians remains debated, especially when balancing oncologic control, renal preservation, and procedural safety. While ablative techniques and active surveillance are often favored in frail patients, robust comparative evidence supporting nephron-sparing surgery in this age group is limited. <b>Methods</b>: We retrospectively reviewed consecutive patients aged ≥80 years who underwent minimally invasive surgery for cT1 clear cell RCC at a high-volume tertiary-care center between July 2001 and August 2025. Patients were stratified into two cohorts: minimally invasive partial nephrectomy (MIPN, <i>n</i> = 51) and radical nephrectomy (MIRN, n = 26). All MIPNs were performed using an off-clamp approach. Baseline, perioperative, functional, and oncologic outcomes were compared. Kaplan-Meier analysis estimated overall survival (OS), cancer-specific survival (CSS), and progression to significant chronic kidney disease (sCKD, defined as CKD stage ≥ 3b). <b>Results</b>: Groups were comparable in age, comorbidities, and ASA score. MIRN patients exhibited higher tumor complexity (RENAL score: 9 vs. 7, <i>p</i> = 0.01) and a greater proportion of pT1b lesions (77% vs. 37.3%, <i>p</i> = 0.01). Perioperative transfusions occurred exclusively in the MIRN group (<i>p</i> = 0.01), whereas complication rates were low and similar between groups. MIPN was associated with significantly higher eGFR at follow-up (48 vs. 30.9 mL/min/1.73 m<sup>2</sup>, <i>p</i> = 0.01) and a delayed progression to sCKD (<i>p</i> = 0.01), with no differences in OS or CSS at a median follow-up of 30.5 months. <b>Conclusions</b>: In this real-world series of ultra-octogenarians with cT1 clear cell RCC, off-clamp minimally invasive partial nephrectomy ensured superior renal function preservation and delayed progression to sCKD, without compromising oncologic control at mid-term follow-up. Beyond statistical outcomes, these results underscore the importance of tailoring surgical strategies to protect long-term functional autonomy and preserve physiological resilience in elderly patients.</p>\",\"PeriodicalId\":15533,\"journal\":{\"name\":\"Journal of Clinical Medicine\",\"volume\":\"14 18\",\"pages\":\"\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-09-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12471238/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/jcm14186634\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcm14186634","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
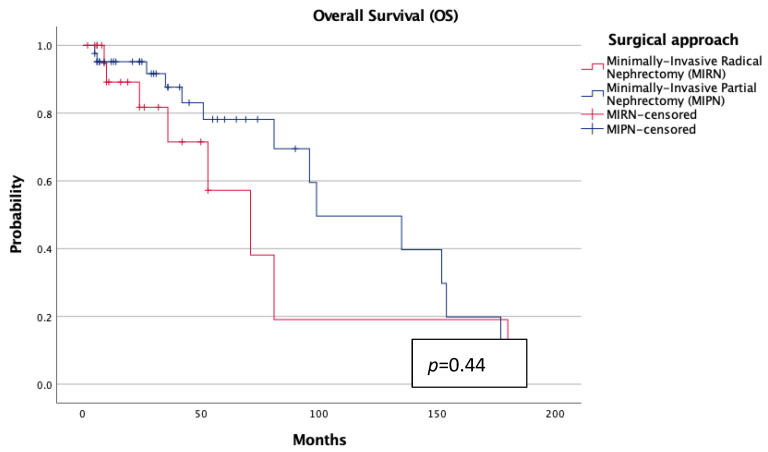
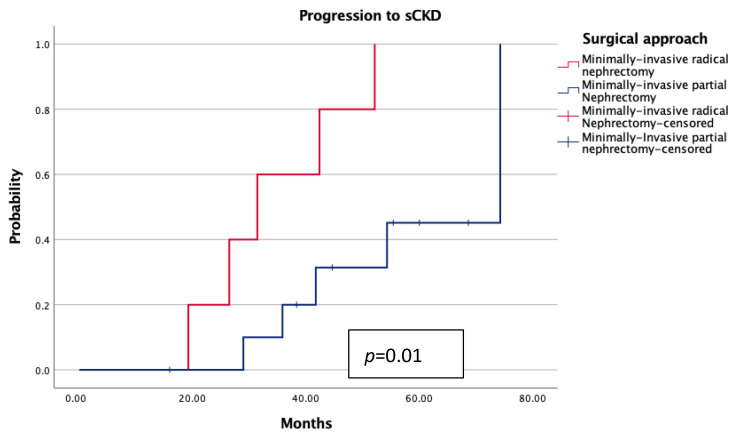
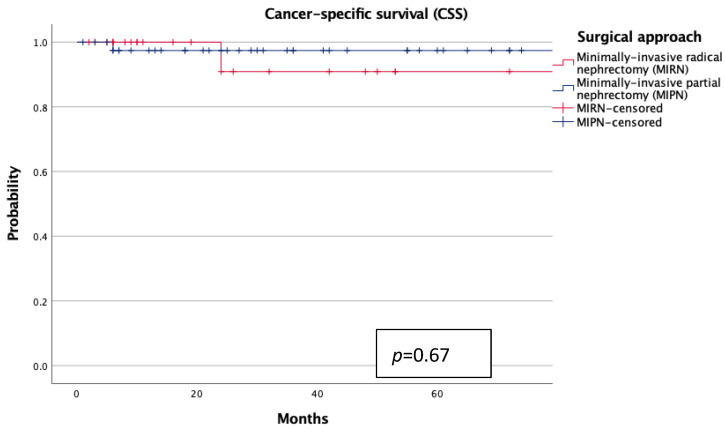
背景/目的:超80岁高龄患者I期肾细胞癌(RCC)的最佳手术入路仍存在争议,特别是在平衡肿瘤控制、肾脏保存和手术安全性方面。虽然消融技术和主动监测通常在虚弱的患者中得到青睐,但在这个年龄组中支持保留肾单元手术的有力的比较证据是有限的。方法:我们回顾性回顾了2001年7月至2025年8月在一家大容量三级医疗中心连续接受微创手术治疗cT1透明细胞RCC的年龄≥80岁的患者。患者被分为两组:微创部分肾切除术(MIPN, n = 51)和根治性肾切除术(MIRN, n = 26)。所有MIPNs均采用脱钳入路。比较基线、围手术期、功能和肿瘤预后。Kaplan-Meier分析估计了总生存期(OS)、癌症特异性生存期(CSS)和进展到显著慢性肾脏疾病(sCKD,定义为CKD分期≥3b)。结果:各组在年龄、合并症和ASA评分方面具有可比性。MIRN患者肿瘤复杂性更高(RENAL评分:9比7,p = 0.01), pT1b病变比例更高(77%比37.3%,p = 0.01)。围手术期输血发生率仅为MIRN组(p = 0.01),两组并发症发生率低且相似。随访时,MIPN与eGFR显著升高(48 vs. 30.9 mL/min/1.73 m2, p = 0.01)和sCKD进展延迟(p = 0.01)相关,中位随访30.5个月时OS或CSS无差异。结论:在这个真实世界的超80岁的cT1透明细胞RCC患者中,非钳形微创部分肾切除术确保了良好的肾功能保存和延迟sCKD的进展,在中期随访中没有影响肿瘤控制。除了统计结果外,这些结果强调了定制手术策略的重要性,以保护老年患者的长期功能自主和保持生理弹性。
Framing Surgical Decisions in Elderly Patients: Minimally Invasive Partial Versus Radical Nephrectomy for Stage I Renal Cell Carcinoma at Mid-Term Follow-Up.
Background/Objectives: The optimal surgical approach for stage I renal cell carcinoma (RCC) in ultra-octogenarians remains debated, especially when balancing oncologic control, renal preservation, and procedural safety. While ablative techniques and active surveillance are often favored in frail patients, robust comparative evidence supporting nephron-sparing surgery in this age group is limited. Methods: We retrospectively reviewed consecutive patients aged ≥80 years who underwent minimally invasive surgery for cT1 clear cell RCC at a high-volume tertiary-care center between July 2001 and August 2025. Patients were stratified into two cohorts: minimally invasive partial nephrectomy (MIPN, n = 51) and radical nephrectomy (MIRN, n = 26). All MIPNs were performed using an off-clamp approach. Baseline, perioperative, functional, and oncologic outcomes were compared. Kaplan-Meier analysis estimated overall survival (OS), cancer-specific survival (CSS), and progression to significant chronic kidney disease (sCKD, defined as CKD stage ≥ 3b). Results: Groups were comparable in age, comorbidities, and ASA score. MIRN patients exhibited higher tumor complexity (RENAL score: 9 vs. 7, p = 0.01) and a greater proportion of pT1b lesions (77% vs. 37.3%, p = 0.01). Perioperative transfusions occurred exclusively in the MIRN group (p = 0.01), whereas complication rates were low and similar between groups. MIPN was associated with significantly higher eGFR at follow-up (48 vs. 30.9 mL/min/1.73 m2, p = 0.01) and a delayed progression to sCKD (p = 0.01), with no differences in OS or CSS at a median follow-up of 30.5 months. Conclusions: In this real-world series of ultra-octogenarians with cT1 clear cell RCC, off-clamp minimally invasive partial nephrectomy ensured superior renal function preservation and delayed progression to sCKD, without compromising oncologic control at mid-term follow-up. Beyond statistical outcomes, these results underscore the importance of tailoring surgical strategies to protect long-term functional autonomy and preserve physiological resilience in elderly patients.
期刊介绍:
Journal of Clinical Medicine (ISSN 2077-0383), is an international scientific open access journal, providing a platform for advances in health care/clinical practices, the study of direct observation of patients and general medical research. This multi-disciplinary journal is aimed at a wide audience of medical researchers and healthcare professionals.
Unique features of this journal:
manuscripts regarding original research and ideas will be particularly welcomed.JCM also accepts reviews, communications, and short notes.
There is no limit to publication length: our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


