Marco Lorenzo Bonù, Giulia Volpi, Gloria Zanni, Jacopo Balduzzi, Fabrizia Terraneo, Giusto Pignata, Giuseppina Arcangeli, Francesco Frassine, Paola Vitali, Eliana La Rocca, Simone Giacopuzzi, Jacopo Weindelmayer, Carlo Alberto De Pasqual, Martina Milazzo, Michele Pavarana, Valentina Zen, Stefano De Pascale, Uberto Fumagalli Romario, Michela Buglione, Giovanni De Manzoni
{"title":"TCF加放化疗、新辅助放化疗、斑块围手术期化疗治疗食管腺癌:一项三队列、多中心比较的结果:A4研究","authors":"Marco Lorenzo Bonù, Giulia Volpi, Gloria Zanni, Jacopo Balduzzi, Fabrizia Terraneo, Giusto Pignata, Giuseppina Arcangeli, Francesco Frassine, Paola Vitali, Eliana La Rocca, Simone Giacopuzzi, Jacopo Weindelmayer, Carlo Alberto De Pasqual, Martina Milazzo, Michele Pavarana, Valentina Zen, Stefano De Pascale, Uberto Fumagalli Romario, Michela Buglione, Giovanni De Manzoni","doi":"10.3390/biomedicines13092236","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> Recent randomized evidence suggests that stage II-IV non metastatic esophageal adenocarcinoma is best managed with perioperative chemotherapy (CHT) and surgery. Intensification of neoadjuvant chemotherapy and radiochemotherapy are proposed before surgery in high-volume centers with the aim of increasing both systemic and locoregional control. However, few data comparing intensified RTCHT, CHT plus RTCHT and perioperative CHT with FLOT in real-life scenarios are available. <b>Methods:</b> This is a multicenter, retrospective series, including three cohorts of patients treated for esophageal adenocarcinoma: Cohort A: nRTCHT; Cohort B: TCF plus RTCHT, defined as triplet chemotherapy followed by dose-reduced triplet therapy + RT; Cohort C: perioperative chemotherapy with FLOT regimen. The primary endpoint was disease-free survival (DFS), and the secondary endpoints were pathologic complete response (pCR), pathologic lymph-node complete response (ypN0), overall survival (OS), and perioperative acute toxicity. <b>Results:</b> From January 2013 to December 2023, 142 patients were identified. All patients received multimodal therapy with radical esophagectomy. A total of 95% of patients were male; the majority of patients presented with stage cT3cN1. A total of 63 patients were treated in Cohort A (31 cases with doublet 5FU-CDDP concurrent to 50.4 Gy and 32 cases with CROSS regimen), 36 in Cohort B, and 43 in Cohort C. After a median FU of 36 months, the 3-year DFS resulted 58.6%. pCR occurred in 26 cases (18.6%). Three-year OS had a value of 72%. At univariate analysis, ypN0 was related to better DFS; cN+ disease was related with worse OS. The treatment cohort did not impact survival outcomes; however, an effect on CR was shown, with pCR in 15% (A), 36.3% (B), 11% (C) of cases, respectively (χ: 0.008). A total of 67% of patients in Cohort B experienced a ypN0. Two treatment-related deaths occurred (one in Cohort A and one in C) with a slight increase in G3 toxicity in cohort C. <b>Conclusions:</b> In this real-life multicenter series, oncological results were adequate for all three neoadjuvant strategies. TCF plus RTCHT guaranteed a higher pCR and ypN0 rate without increasing toxicity. An intensified neoadjuvant schedule, such as TCF plus RTCHT, may be useful in cases where higher tumor and nodal responses are needed. Taken together, our data highlight that further investigation is warranted before abandoning radiotherapy-based neoadjuvant approaches in esophageal and GEJ adenocarcinoma.</p>","PeriodicalId":8937,"journal":{"name":"Biomedicines","volume":"13 9","pages":""},"PeriodicalIF":3.9000,"publicationDate":"2025-09-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12467824/pdf/","citationCount":"0","resultStr":"{\"title\":\"TCF Plus Radiochemotherapy Versus Neoadjuvant Radiochemotherapy Versus Flot Perioperative Chemotherapy in Esophageal Adenocarcinoma: The Results of a Three-Cohort, Multi-Centric Comparison: The A4 Study.\",\"authors\":\"Marco Lorenzo Bonù, Giulia Volpi, Gloria Zanni, Jacopo Balduzzi, Fabrizia Terraneo, Giusto Pignata, Giuseppina Arcangeli, Francesco Frassine, Paola Vitali, Eliana La Rocca, Simone Giacopuzzi, Jacopo Weindelmayer, Carlo Alberto De Pasqual, Martina Milazzo, Michele Pavarana, Valentina Zen, Stefano De Pascale, Uberto Fumagalli Romario, Michela Buglione, Giovanni De Manzoni\",\"doi\":\"10.3390/biomedicines13092236\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction:</b> Recent randomized evidence suggests that stage II-IV non metastatic esophageal adenocarcinoma is best managed with perioperative chemotherapy (CHT) and surgery. Intensification of neoadjuvant chemotherapy and radiochemotherapy are proposed before surgery in high-volume centers with the aim of increasing both systemic and locoregional control. However, few data comparing intensified RTCHT, CHT plus RTCHT and perioperative CHT with FLOT in real-life scenarios are available. <b>Methods:</b> This is a multicenter, retrospective series, including three cohorts of patients treated for esophageal adenocarcinoma: Cohort A: nRTCHT; Cohort B: TCF plus RTCHT, defined as triplet chemotherapy followed by dose-reduced triplet therapy + RT; Cohort C: perioperative chemotherapy with FLOT regimen. The primary endpoint was disease-free survival (DFS), and the secondary endpoints were pathologic complete response (pCR), pathologic lymph-node complete response (ypN0), overall survival (OS), and perioperative acute toxicity. <b>Results:</b> From January 2013 to December 2023, 142 patients were identified. All patients received multimodal therapy with radical esophagectomy. A total of 95% of patients were male; the majority of patients presented with stage cT3cN1. A total of 63 patients were treated in Cohort A (31 cases with doublet 5FU-CDDP concurrent to 50.4 Gy and 32 cases with CROSS regimen), 36 in Cohort B, and 43 in Cohort C. After a median FU of 36 months, the 3-year DFS resulted 58.6%. pCR occurred in 26 cases (18.6%). Three-year OS had a value of 72%. At univariate analysis, ypN0 was related to better DFS; cN+ disease was related with worse OS. The treatment cohort did not impact survival outcomes; however, an effect on CR was shown, with pCR in 15% (A), 36.3% (B), 11% (C) of cases, respectively (χ: 0.008). A total of 67% of patients in Cohort B experienced a ypN0. Two treatment-related deaths occurred (one in Cohort A and one in C) with a slight increase in G3 toxicity in cohort C. <b>Conclusions:</b> In this real-life multicenter series, oncological results were adequate for all three neoadjuvant strategies. TCF plus RTCHT guaranteed a higher pCR and ypN0 rate without increasing toxicity. An intensified neoadjuvant schedule, such as TCF plus RTCHT, may be useful in cases where higher tumor and nodal responses are needed. Taken together, our data highlight that further investigation is warranted before abandoning radiotherapy-based neoadjuvant approaches in esophageal and GEJ adenocarcinoma.</p>\",\"PeriodicalId\":8937,\"journal\":{\"name\":\"Biomedicines\",\"volume\":\"13 9\",\"pages\":\"\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2025-09-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12467824/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biomedicines\",\"FirstCategoryId\":\"5\",\"ListUrlMain\":\"https://doi.org/10.3390/biomedicines13092236\",\"RegionNum\":3,\"RegionCategory\":\"工程技术\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"BIOCHEMISTRY & MOLECULAR BIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomedicines","FirstCategoryId":"5","ListUrlMain":"https://doi.org/10.3390/biomedicines13092236","RegionNum":3,"RegionCategory":"工程技术","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
TCF Plus Radiochemotherapy Versus Neoadjuvant Radiochemotherapy Versus Flot Perioperative Chemotherapy in Esophageal Adenocarcinoma: The Results of a Three-Cohort, Multi-Centric Comparison: The A4 Study.
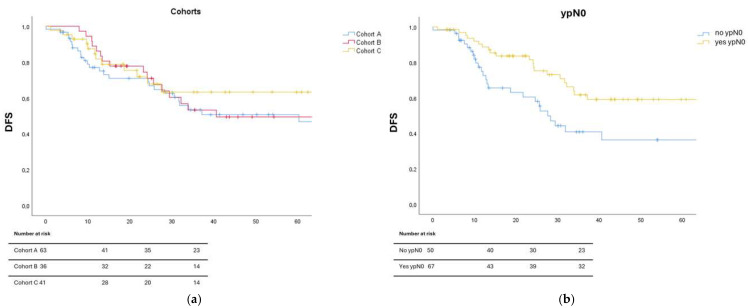
Introduction: Recent randomized evidence suggests that stage II-IV non metastatic esophageal adenocarcinoma is best managed with perioperative chemotherapy (CHT) and surgery. Intensification of neoadjuvant chemotherapy and radiochemotherapy are proposed before surgery in high-volume centers with the aim of increasing both systemic and locoregional control. However, few data comparing intensified RTCHT, CHT plus RTCHT and perioperative CHT with FLOT in real-life scenarios are available. Methods: This is a multicenter, retrospective series, including three cohorts of patients treated for esophageal adenocarcinoma: Cohort A: nRTCHT; Cohort B: TCF plus RTCHT, defined as triplet chemotherapy followed by dose-reduced triplet therapy + RT; Cohort C: perioperative chemotherapy with FLOT regimen. The primary endpoint was disease-free survival (DFS), and the secondary endpoints were pathologic complete response (pCR), pathologic lymph-node complete response (ypN0), overall survival (OS), and perioperative acute toxicity. Results: From January 2013 to December 2023, 142 patients were identified. All patients received multimodal therapy with radical esophagectomy. A total of 95% of patients were male; the majority of patients presented with stage cT3cN1. A total of 63 patients were treated in Cohort A (31 cases with doublet 5FU-CDDP concurrent to 50.4 Gy and 32 cases with CROSS regimen), 36 in Cohort B, and 43 in Cohort C. After a median FU of 36 months, the 3-year DFS resulted 58.6%. pCR occurred in 26 cases (18.6%). Three-year OS had a value of 72%. At univariate analysis, ypN0 was related to better DFS; cN+ disease was related with worse OS. The treatment cohort did not impact survival outcomes; however, an effect on CR was shown, with pCR in 15% (A), 36.3% (B), 11% (C) of cases, respectively (χ: 0.008). A total of 67% of patients in Cohort B experienced a ypN0. Two treatment-related deaths occurred (one in Cohort A and one in C) with a slight increase in G3 toxicity in cohort C. Conclusions: In this real-life multicenter series, oncological results were adequate for all three neoadjuvant strategies. TCF plus RTCHT guaranteed a higher pCR and ypN0 rate without increasing toxicity. An intensified neoadjuvant schedule, such as TCF plus RTCHT, may be useful in cases where higher tumor and nodal responses are needed. Taken together, our data highlight that further investigation is warranted before abandoning radiotherapy-based neoadjuvant approaches in esophageal and GEJ adenocarcinoma.
BiomedicinesBiochemistry, Genetics and Molecular Biology-General Biochemistry,Genetics and Molecular Biology
CiteScore
5.20
自引率
8.50%
发文量
2823
审稿时长
8 weeks
期刊介绍:
Biomedicines (ISSN 2227-9059; CODEN: BIOMID) is an international, scientific, open access journal on biomedicines published quarterly online by MDPI.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


