Yoshinori Tsubakimoto, Jun Shiraishi, Daisuke Usuki, Shin Takiuchi, Satoru Otsuji
{"title":"经侧支腘下血管重建术的有效性和安全性:一项单中心回顾性研究。","authors":"Yoshinori Tsubakimoto, Jun Shiraishi, Daisuke Usuki, Shin Takiuchi, Satoru Otsuji","doi":"10.1186/s42155-025-00595-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endovascular therapy (EVT) has become a key revascularization strategy for patients with chronic limb-threatening ischemia (CLTI), especially in cases involving infrapopliteal (IP) chronic total occlusions (CTOs), which are often challenging to treat using standard antegrade approaches alone. Trans-collateral angioplasty (TCA) is a retrograde technique that accesses the distal true lumen via collateral vessels when conventional methods are unsuccessful. However, clinical evidence regarding the efficacy and safety of TCA remains insufficient. This study aimed to evaluate the efficacy and safety of TCA as a retrograde approach during EVT for IP CTO lesions.</p><p><strong>Results: </strong>This retrospective single-center study included 44 IP CTO lesions in patients who underwent TCA between January 2020 and December 2022, after excluding 18 lesions treated solely with the pedal-plantar loop technique. The mean patient age was 78.8 years, and 81.8% had diabetes, 79.5% had chronic kidney disease, and 31.8% were on dialysis. EVT success was achieved in 95.5% (95% CI: 84.9-98.7) of lesions. TCA alone achieved lesion crossing in 70.5% (95% CI: 55.8-81.8), while distal puncture was required in 13.6% (95% CI: 6.4-27.0) of cases. Various crossing techniques, including the rendezvous technique and reverse subintimal tracking, were conducted. Collateral vessel-related complications occurred in 11.3% (5 lesions; 95% CI: 5.0-24.6), including injury in 6.8%, and occlusion and spasm in 2.3%. No vessel dissections occurred. The overall incidence of perioperative complications within 30 days was 20.5% (95% CI: 11.3-34.2), most commonly gastrointestinal bleeding and stroke. At one year, the rate of freedom from target lesion revascularization was 45.4%, and amputation-free survival was 84.0%.</p><p><strong>Conclusions: </strong>Our findings suggest that TCA can be a feasible and relatively safe retrograde strategy for complex IP CTO lesions when antegrade wiring fails. It is associated with high procedural success and a low incidence of collateral vessel-related complications, supporting its use in selected cases of CLTI.</p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":"8 1","pages":"72"},"PeriodicalIF":1.5000,"publicationDate":"2025-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474752/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy and safety of Trans-collateral revascularization of infrapopliteal vessels: A Single-center retrospective study.\",\"authors\":\"Yoshinori Tsubakimoto, Jun Shiraishi, Daisuke Usuki, Shin Takiuchi, Satoru Otsuji\",\"doi\":\"10.1186/s42155-025-00595-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Endovascular therapy (EVT) has become a key revascularization strategy for patients with chronic limb-threatening ischemia (CLTI), especially in cases involving infrapopliteal (IP) chronic total occlusions (CTOs), which are often challenging to treat using standard antegrade approaches alone. Trans-collateral angioplasty (TCA) is a retrograde technique that accesses the distal true lumen via collateral vessels when conventional methods are unsuccessful. However, clinical evidence regarding the efficacy and safety of TCA remains insufficient. This study aimed to evaluate the efficacy and safety of TCA as a retrograde approach during EVT for IP CTO lesions.</p><p><strong>Results: </strong>This retrospective single-center study included 44 IP CTO lesions in patients who underwent TCA between January 2020 and December 2022, after excluding 18 lesions treated solely with the pedal-plantar loop technique. The mean patient age was 78.8 years, and 81.8% had diabetes, 79.5% had chronic kidney disease, and 31.8% were on dialysis. EVT success was achieved in 95.5% (95% CI: 84.9-98.7) of lesions. TCA alone achieved lesion crossing in 70.5% (95% CI: 55.8-81.8), while distal puncture was required in 13.6% (95% CI: 6.4-27.0) of cases. Various crossing techniques, including the rendezvous technique and reverse subintimal tracking, were conducted. Collateral vessel-related complications occurred in 11.3% (5 lesions; 95% CI: 5.0-24.6), including injury in 6.8%, and occlusion and spasm in 2.3%. No vessel dissections occurred. The overall incidence of perioperative complications within 30 days was 20.5% (95% CI: 11.3-34.2), most commonly gastrointestinal bleeding and stroke. At one year, the rate of freedom from target lesion revascularization was 45.4%, and amputation-free survival was 84.0%.</p><p><strong>Conclusions: </strong>Our findings suggest that TCA can be a feasible and relatively safe retrograde strategy for complex IP CTO lesions when antegrade wiring fails. It is associated with high procedural success and a low incidence of collateral vessel-related complications, supporting its use in selected cases of CLTI.</p>\",\"PeriodicalId\":52351,\"journal\":{\"name\":\"CVIR Endovascular\",\"volume\":\"8 1\",\"pages\":\"72\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-09-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474752/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CVIR Endovascular\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s42155-025-00595-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-025-00595-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Efficacy and safety of Trans-collateral revascularization of infrapopliteal vessels: A Single-center retrospective study.
Background: Endovascular therapy (EVT) has become a key revascularization strategy for patients with chronic limb-threatening ischemia (CLTI), especially in cases involving infrapopliteal (IP) chronic total occlusions (CTOs), which are often challenging to treat using standard antegrade approaches alone. Trans-collateral angioplasty (TCA) is a retrograde technique that accesses the distal true lumen via collateral vessels when conventional methods are unsuccessful. However, clinical evidence regarding the efficacy and safety of TCA remains insufficient. This study aimed to evaluate the efficacy and safety of TCA as a retrograde approach during EVT for IP CTO lesions.
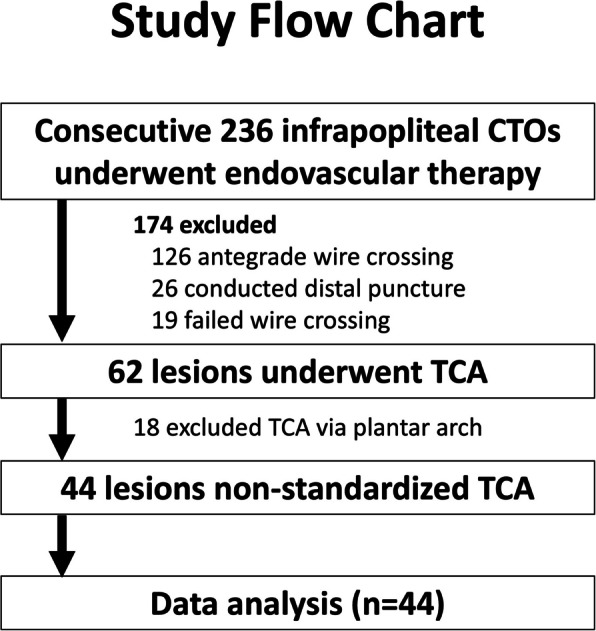
Results: This retrospective single-center study included 44 IP CTO lesions in patients who underwent TCA between January 2020 and December 2022, after excluding 18 lesions treated solely with the pedal-plantar loop technique. The mean patient age was 78.8 years, and 81.8% had diabetes, 79.5% had chronic kidney disease, and 31.8% were on dialysis. EVT success was achieved in 95.5% (95% CI: 84.9-98.7) of lesions. TCA alone achieved lesion crossing in 70.5% (95% CI: 55.8-81.8), while distal puncture was required in 13.6% (95% CI: 6.4-27.0) of cases. Various crossing techniques, including the rendezvous technique and reverse subintimal tracking, were conducted. Collateral vessel-related complications occurred in 11.3% (5 lesions; 95% CI: 5.0-24.6), including injury in 6.8%, and occlusion and spasm in 2.3%. No vessel dissections occurred. The overall incidence of perioperative complications within 30 days was 20.5% (95% CI: 11.3-34.2), most commonly gastrointestinal bleeding and stroke. At one year, the rate of freedom from target lesion revascularization was 45.4%, and amputation-free survival was 84.0%.
Conclusions: Our findings suggest that TCA can be a feasible and relatively safe retrograde strategy for complex IP CTO lesions when antegrade wiring fails. It is associated with high procedural success and a low incidence of collateral vessel-related complications, supporting its use in selected cases of CLTI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


