Maciej Dyrbuś, Łukasz Pyka, Anna Kurek, Jacek Niedziela, Elżbieta Adamowicz-Czoch, Katarzyna Sokoła, Joanna Machowicz, Mateusz Ostręga, Damian Pres, Michał Skrzypek, Mariusz Gąsior, Mateusz Tajstra
{"title":"发电机更换后植入式心律转复除颤器治疗-长期远程监测数据。","authors":"Maciej Dyrbuś, Łukasz Pyka, Anna Kurek, Jacek Niedziela, Elżbieta Adamowicz-Czoch, Katarzyna Sokoła, Joanna Machowicz, Mateusz Ostręga, Damian Pres, Michał Skrzypek, Mariusz Gąsior, Mateusz Tajstra","doi":"10.3390/clinpract15090160","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: The rate of long-term outcomes, including arrhythmic episodes following implantable cardioverter-defibrillator (ICD) device replacements, is often unknown. Thus, the aim of this manuscript was to evaluate the risk of ICD or cardiac resynchronization therapy-defibrillator (CRT-D) therapies in remotely monitored patients following device replacement. <b>Methods</b>: Data from 134 patients who underwent ICD/CRT-D replacement or upgrade were analyzed. Kaplan-Meier estimates, as well as Cox proportional hazards regression, were used to present long-term outcomes and predictors of study endpoints, these being all-cause mortality, and appropriate and inappropriate ICD/CRT-D therapies. <b>Results</b>: Among the cohort, 51.5% of patients received ICDs and 48.5% received CRT-Ds; the median (quartile 1-quartile 3) LVEF at replacement was 23.0% (18.0-28.0%). In 11 (8.2%) patients, the LVEF at replacement was higher than 35%. During the median (Q1-Q3) follow-up of 3.0 (1.4-5.0) years, 32.1% experienced appropriate and 6.0% experienced inappropriate therapies. The all-cause mortality rate was 38.0%, and appropriate antitachycardia pacing (ATP), a reduced baseline LVEF, and no history of myocardial infarction were independent predictors of death (odds ratios of 1.87 for appropriate ATP, 0.88 per 1% of the LVEF and 0.54 for a history of MI, respectively). The rate of appropriate device therapies was numerically lower in patients whose LVEF improved (19.8% vs. 33.3% and 0% vs. 6.5%, for appropriate and inappropriate therapies). An LVEF of >35% at replacement did not influence the analyzed outcomes. <b>Conclusions</b>: In patients who underwent ICD/CRT-D replacement, an improvement in LVEF was not identified as either a predictor of improved survival or of a lower risk of needing device therapies. Further stratification models are needed to evaluate the arrhythmic risk in patients after generator replacements.</p>","PeriodicalId":45306,"journal":{"name":"Clinics and Practice","volume":"15 9","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2025-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12468052/pdf/","citationCount":"0","resultStr":"{\"title\":\"Implantable Cardioverter-Defibrillator Therapies Following Generator Replacements-Long-Term Remote Monitoring Data.\",\"authors\":\"Maciej Dyrbuś, Łukasz Pyka, Anna Kurek, Jacek Niedziela, Elżbieta Adamowicz-Czoch, Katarzyna Sokoła, Joanna Machowicz, Mateusz Ostręga, Damian Pres, Michał Skrzypek, Mariusz Gąsior, Mateusz Tajstra\",\"doi\":\"10.3390/clinpract15090160\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background</b>: The rate of long-term outcomes, including arrhythmic episodes following implantable cardioverter-defibrillator (ICD) device replacements, is often unknown. Thus, the aim of this manuscript was to evaluate the risk of ICD or cardiac resynchronization therapy-defibrillator (CRT-D) therapies in remotely monitored patients following device replacement. <b>Methods</b>: Data from 134 patients who underwent ICD/CRT-D replacement or upgrade were analyzed. Kaplan-Meier estimates, as well as Cox proportional hazards regression, were used to present long-term outcomes and predictors of study endpoints, these being all-cause mortality, and appropriate and inappropriate ICD/CRT-D therapies. <b>Results</b>: Among the cohort, 51.5% of patients received ICDs and 48.5% received CRT-Ds; the median (quartile 1-quartile 3) LVEF at replacement was 23.0% (18.0-28.0%). In 11 (8.2%) patients, the LVEF at replacement was higher than 35%. During the median (Q1-Q3) follow-up of 3.0 (1.4-5.0) years, 32.1% experienced appropriate and 6.0% experienced inappropriate therapies. The all-cause mortality rate was 38.0%, and appropriate antitachycardia pacing (ATP), a reduced baseline LVEF, and no history of myocardial infarction were independent predictors of death (odds ratios of 1.87 for appropriate ATP, 0.88 per 1% of the LVEF and 0.54 for a history of MI, respectively). The rate of appropriate device therapies was numerically lower in patients whose LVEF improved (19.8% vs. 33.3% and 0% vs. 6.5%, for appropriate and inappropriate therapies). An LVEF of >35% at replacement did not influence the analyzed outcomes. <b>Conclusions</b>: In patients who underwent ICD/CRT-D replacement, an improvement in LVEF was not identified as either a predictor of improved survival or of a lower risk of needing device therapies. Further stratification models are needed to evaluate the arrhythmic risk in patients after generator replacements.</p>\",\"PeriodicalId\":45306,\"journal\":{\"name\":\"Clinics and Practice\",\"volume\":\"15 9\",\"pages\":\"\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-08-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12468052/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinics and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/clinpract15090160\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/clinpract15090160","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Implantable Cardioverter-Defibrillator Therapies Following Generator Replacements-Long-Term Remote Monitoring Data.
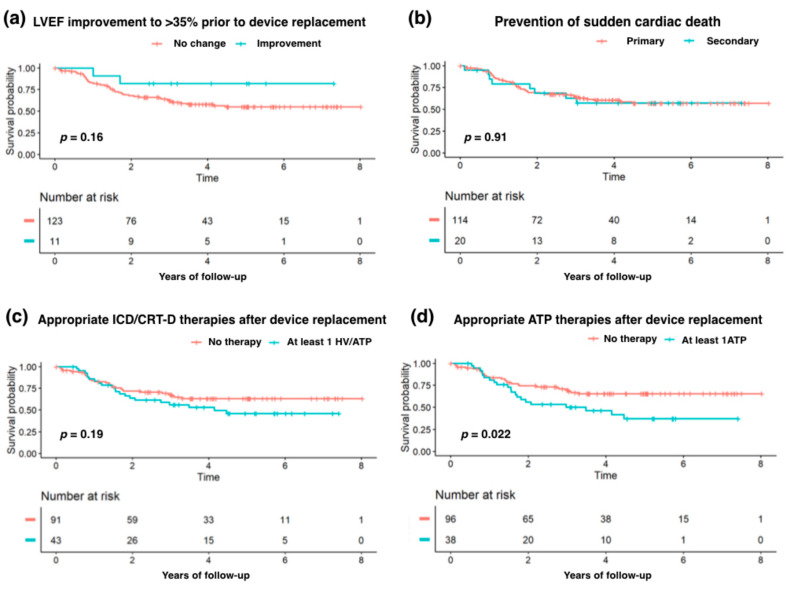
Background: The rate of long-term outcomes, including arrhythmic episodes following implantable cardioverter-defibrillator (ICD) device replacements, is often unknown. Thus, the aim of this manuscript was to evaluate the risk of ICD or cardiac resynchronization therapy-defibrillator (CRT-D) therapies in remotely monitored patients following device replacement. Methods: Data from 134 patients who underwent ICD/CRT-D replacement or upgrade were analyzed. Kaplan-Meier estimates, as well as Cox proportional hazards regression, were used to present long-term outcomes and predictors of study endpoints, these being all-cause mortality, and appropriate and inappropriate ICD/CRT-D therapies. Results: Among the cohort, 51.5% of patients received ICDs and 48.5% received CRT-Ds; the median (quartile 1-quartile 3) LVEF at replacement was 23.0% (18.0-28.0%). In 11 (8.2%) patients, the LVEF at replacement was higher than 35%. During the median (Q1-Q3) follow-up of 3.0 (1.4-5.0) years, 32.1% experienced appropriate and 6.0% experienced inappropriate therapies. The all-cause mortality rate was 38.0%, and appropriate antitachycardia pacing (ATP), a reduced baseline LVEF, and no history of myocardial infarction were independent predictors of death (odds ratios of 1.87 for appropriate ATP, 0.88 per 1% of the LVEF and 0.54 for a history of MI, respectively). The rate of appropriate device therapies was numerically lower in patients whose LVEF improved (19.8% vs. 33.3% and 0% vs. 6.5%, for appropriate and inappropriate therapies). An LVEF of >35% at replacement did not influence the analyzed outcomes. Conclusions: In patients who underwent ICD/CRT-D replacement, an improvement in LVEF was not identified as either a predictor of improved survival or of a lower risk of needing device therapies. Further stratification models are needed to evaluate the arrhythmic risk in patients after generator replacements.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


