{"title":"颈动脉ct血管造影显示的小斑块与来源不明的栓塞性卒中的关系。","authors":"Junpei Nagasawa, Tatsuhiro Yokoyama, Makiko Ogawa, Ryuichi Okamoto, Mari Shibukawa, Junya Ebina, Takehisa Hirayama, Osamu Kano","doi":"10.3390/neurolint17090148","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objectives</b>: While traditionally, carotid plaques with significant stenosis have been considered major embolic sources, recent evidence suggests that even non-stenotic small plaques with a <50% stenosis rate may contribute to cerebral infarction. Herein, we evaluated the relationship between non-stenotic small plaques and embolic stroke of undetermined source (ESUS) using computed tomography angiography (CTA). <b>Materials and Methods</b>: We retrospectively reviewed our single-institutional database of hospitalized patients with stroke between April 2017 and December 2022 and enrolled them with ESUS. We evaluated the presence or absence of non-stenotic carotid artery plaque lesions ipsilateral and contralateral to the cerebral infarction lesion using CTA. A neurologist, blinded to the stroke side and all other clinical information, reviewed each CTA and viewed the axial and sagittal CTA source images. In each image, a line perpendicular to the vessel wall was drawn and the plaque diameter was measured. The largest part was considered as the maximum plaque diameter. <b>Results</b>: A total of 951 patients with stroke were hospitalized during the study period. Among these, 35 patients with unilateral anterior circulation ESUS were enrolled. Plaque prevalence > 3 mm was compared between the carotid artery on the ESUS side and contralateral carotid artery. The prevalences were 31% and 8% on the ESUS and contralateral sides, respectively. Plaques > 3 mm were often found on the ESUS side. <b>Conclusions</b>: Patients with ESUS were more likely to exhibit non-stenotic plaques of ≥3 mm in the infarcted carotid artery than in the contralateral carotid artery. Thus, small non-stenotic plaques may be the embolization source in ESUS, and CT angiography is useful for these evaluations.</p>","PeriodicalId":19130,"journal":{"name":"Neurology International","volume":"17 9","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-09-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12472282/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association Between Carotid Artery Small Plaque on Computed Tomography Angiography and Embolic Stroke of Undetermined Source.\",\"authors\":\"Junpei Nagasawa, Tatsuhiro Yokoyama, Makiko Ogawa, Ryuichi Okamoto, Mari Shibukawa, Junya Ebina, Takehisa Hirayama, Osamu Kano\",\"doi\":\"10.3390/neurolint17090148\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Objectives</b>: While traditionally, carotid plaques with significant stenosis have been considered major embolic sources, recent evidence suggests that even non-stenotic small plaques with a <50% stenosis rate may contribute to cerebral infarction. Herein, we evaluated the relationship between non-stenotic small plaques and embolic stroke of undetermined source (ESUS) using computed tomography angiography (CTA). <b>Materials and Methods</b>: We retrospectively reviewed our single-institutional database of hospitalized patients with stroke between April 2017 and December 2022 and enrolled them with ESUS. We evaluated the presence or absence of non-stenotic carotid artery plaque lesions ipsilateral and contralateral to the cerebral infarction lesion using CTA. A neurologist, blinded to the stroke side and all other clinical information, reviewed each CTA and viewed the axial and sagittal CTA source images. In each image, a line perpendicular to the vessel wall was drawn and the plaque diameter was measured. The largest part was considered as the maximum plaque diameter. <b>Results</b>: A total of 951 patients with stroke were hospitalized during the study period. Among these, 35 patients with unilateral anterior circulation ESUS were enrolled. Plaque prevalence > 3 mm was compared between the carotid artery on the ESUS side and contralateral carotid artery. The prevalences were 31% and 8% on the ESUS and contralateral sides, respectively. Plaques > 3 mm were often found on the ESUS side. <b>Conclusions</b>: Patients with ESUS were more likely to exhibit non-stenotic plaques of ≥3 mm in the infarcted carotid artery than in the contralateral carotid artery. Thus, small non-stenotic plaques may be the embolization source in ESUS, and CT angiography is useful for these evaluations.</p>\",\"PeriodicalId\":19130,\"journal\":{\"name\":\"Neurology International\",\"volume\":\"17 9\",\"pages\":\"\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-09-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12472282/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/neurolint17090148\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/neurolint17090148","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Association Between Carotid Artery Small Plaque on Computed Tomography Angiography and Embolic Stroke of Undetermined Source.
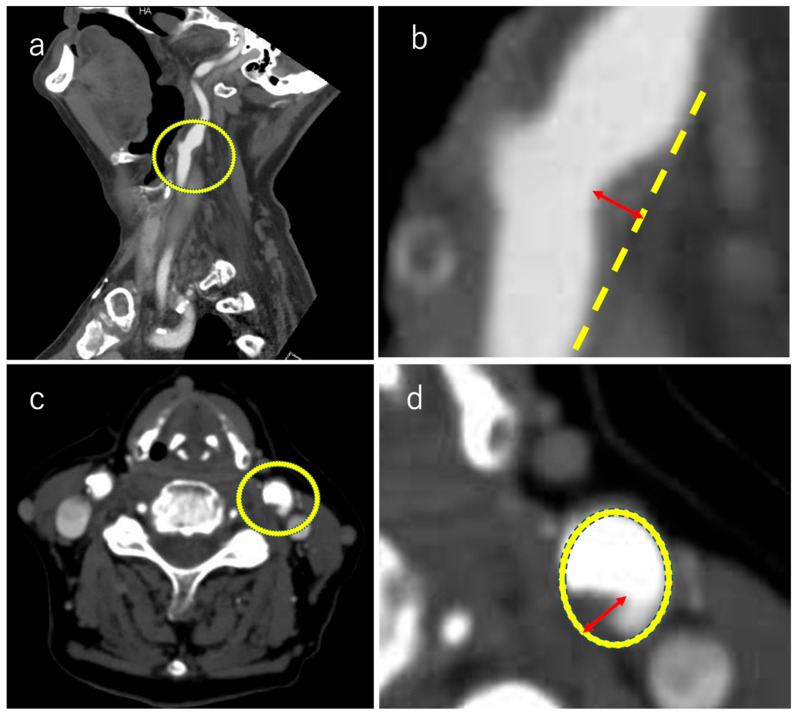
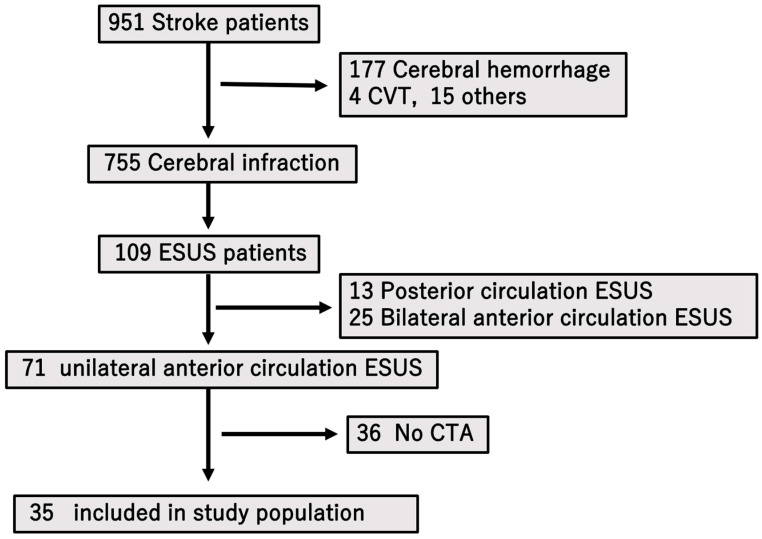
Objectives: While traditionally, carotid plaques with significant stenosis have been considered major embolic sources, recent evidence suggests that even non-stenotic small plaques with a <50% stenosis rate may contribute to cerebral infarction. Herein, we evaluated the relationship between non-stenotic small plaques and embolic stroke of undetermined source (ESUS) using computed tomography angiography (CTA). Materials and Methods: We retrospectively reviewed our single-institutional database of hospitalized patients with stroke between April 2017 and December 2022 and enrolled them with ESUS. We evaluated the presence or absence of non-stenotic carotid artery plaque lesions ipsilateral and contralateral to the cerebral infarction lesion using CTA. A neurologist, blinded to the stroke side and all other clinical information, reviewed each CTA and viewed the axial and sagittal CTA source images. In each image, a line perpendicular to the vessel wall was drawn and the plaque diameter was measured. The largest part was considered as the maximum plaque diameter. Results: A total of 951 patients with stroke were hospitalized during the study period. Among these, 35 patients with unilateral anterior circulation ESUS were enrolled. Plaque prevalence > 3 mm was compared between the carotid artery on the ESUS side and contralateral carotid artery. The prevalences were 31% and 8% on the ESUS and contralateral sides, respectively. Plaques > 3 mm were often found on the ESUS side. Conclusions: Patients with ESUS were more likely to exhibit non-stenotic plaques of ≥3 mm in the infarcted carotid artery than in the contralateral carotid artery. Thus, small non-stenotic plaques may be the embolization source in ESUS, and CT angiography is useful for these evaluations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


