Filipe André Gonzalez, Jacobo Bacariza, Ana Rita Varudo, João Leote, Ricardo Meireles Mateus, Cristina Maia Martins, Maria Inês Ribeiro, Filippo Sanfilippo, Luís Rocha Lopes, Ana G Almeida
{"title":"用应变与非应变超声心动图参数诊断败血症引起的心肌功能障碍:发病率、演变及其与预后的关系。","authors":"Filipe André Gonzalez, Jacobo Bacariza, Ana Rita Varudo, João Leote, Ricardo Meireles Mateus, Cristina Maia Martins, Maria Inês Ribeiro, Filippo Sanfilippo, Luís Rocha Lopes, Ana G Almeida","doi":"10.1186/s13613-025-01561-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sepsis-induced myocardial dysfunction (SIMD) remains poorly defined due to scarce longitudinal studies with advanced echocardiography. We characterized SIMD progression using speckle tracking echocardiography (STE).</p><p><strong>Methods: </strong>Prospective single-center study in septic shock patients admitted to intensive care. SIMD was defined as any left ventricular (LV, systolic and/or diastolic) and/or right ventricular (RV) systolic dysfunction, using STE or non-STE criteria, on days 1, 7 and 30. We studied prevalence, evolution and prognosis of SIMD classified with either criteria using Cox regression.</p><p><strong>Results: </strong>Ninety-eight consecutive patients were included. On day 1, SIMD was identified in n = 57/98 (58.2%) and n = 70/98 (71.4%;p = 0.072) by non-STE and STE parameters, respectively. No significant difference in diagnosis was seen for LV diastolic dysfunction: n = 50/98 (51.0%, non-STE) vs. n = 51/98 (52.0%, STE; p = 1.00). Prevalences of LV and RV systolic dysfunction were not significantly higher with STE criteria: n = 59/98 (60.2%, STE) vs. n = 47/98 (48.0%, non-STE; p = 0.115) for LV; n = 39/98 (39.8%, STE) vs. n = 27/98 (27.6%, non-STE; p = 0.096) for RV. More patients recovered from SIMD when evaluated with non-STE criteria at day 7 (35.3% vs. 17.5% STE; p = 0.033), but not at day 30 (24.5% vs. 18.8% STE; p = 0.501). The 30-day mortality (n = 33/98, 33.7%) was associated with SIMD diagnosed using non-STE (p = 0.010), but not with STE (p = 0.057). In Cox regression, only LVDD by non-STE criteria predicted 30-day mortality (p = 0.005).</p><p><strong>Conclusions: </strong>The incidence of SIMD in septic shock is higher when using STE criteria, with lower reversibility in the first week. A broad definition of SIMD utilizing STE criteria does not seem to provide additional prognostic value.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov: NCT05552521 registered on the 20th of September 2022.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"141"},"PeriodicalIF":5.5000,"publicationDate":"2025-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12463772/pdf/","citationCount":"0","resultStr":"{\"title\":\"Sepsis-induced myocardial dysfunction diagnosed with strain versus non-strain echocardiography parameters: incidence, evolution and association with prognosis.\",\"authors\":\"Filipe André Gonzalez, Jacobo Bacariza, Ana Rita Varudo, João Leote, Ricardo Meireles Mateus, Cristina Maia Martins, Maria Inês Ribeiro, Filippo Sanfilippo, Luís Rocha Lopes, Ana G Almeida\",\"doi\":\"10.1186/s13613-025-01561-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Sepsis-induced myocardial dysfunction (SIMD) remains poorly defined due to scarce longitudinal studies with advanced echocardiography. We characterized SIMD progression using speckle tracking echocardiography (STE).</p><p><strong>Methods: </strong>Prospective single-center study in septic shock patients admitted to intensive care. SIMD was defined as any left ventricular (LV, systolic and/or diastolic) and/or right ventricular (RV) systolic dysfunction, using STE or non-STE criteria, on days 1, 7 and 30. We studied prevalence, evolution and prognosis of SIMD classified with either criteria using Cox regression.</p><p><strong>Results: </strong>Ninety-eight consecutive patients were included. On day 1, SIMD was identified in n = 57/98 (58.2%) and n = 70/98 (71.4%;p = 0.072) by non-STE and STE parameters, respectively. No significant difference in diagnosis was seen for LV diastolic dysfunction: n = 50/98 (51.0%, non-STE) vs. n = 51/98 (52.0%, STE; p = 1.00). Prevalences of LV and RV systolic dysfunction were not significantly higher with STE criteria: n = 59/98 (60.2%, STE) vs. n = 47/98 (48.0%, non-STE; p = 0.115) for LV; n = 39/98 (39.8%, STE) vs. n = 27/98 (27.6%, non-STE; p = 0.096) for RV. More patients recovered from SIMD when evaluated with non-STE criteria at day 7 (35.3% vs. 17.5% STE; p = 0.033), but not at day 30 (24.5% vs. 18.8% STE; p = 0.501). The 30-day mortality (n = 33/98, 33.7%) was associated with SIMD diagnosed using non-STE (p = 0.010), but not with STE (p = 0.057). In Cox regression, only LVDD by non-STE criteria predicted 30-day mortality (p = 0.005).</p><p><strong>Conclusions: </strong>The incidence of SIMD in septic shock is higher when using STE criteria, with lower reversibility in the first week. A broad definition of SIMD utilizing STE criteria does not seem to provide additional prognostic value.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov: NCT05552521 registered on the 20th of September 2022.</p>\",\"PeriodicalId\":7966,\"journal\":{\"name\":\"Annals of Intensive Care\",\"volume\":\"15 1\",\"pages\":\"141\"},\"PeriodicalIF\":5.5000,\"publicationDate\":\"2025-09-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12463772/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13613-025-01561-w\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01561-w","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:由于缺乏先进超声心动图的纵向研究,脓毒症诱发的心肌功能障碍(SIMD)仍然定义不清。我们使用斑点跟踪超声心动图(STE)来描述SIMD的进展。方法:对重症监护的感染性休克患者进行前瞻性单中心研究。SIMD被定义为任何左心室(LV、收缩和/或舒张)和/或右心室(RV)收缩功能障碍,使用STE或非STE标准,在第1、7和30天。我们使用Cox回归研究了SIMD的患病率、演变和预后。结果:连续纳入98例患者。第1天,通过非STE和STE参数分别鉴定出n = 57/98(58.2%)和n = 70/98 (71.4%, p = 0.072)的SIMD。左室舒张功能障碍的诊断无显著差异:n = 50/98(51.0%,非STE) vs. n = 51/98 (52.0%, STE; p = 1.00)。STE标准下左室和右室收缩功能障碍的患病率没有显著升高:左室n = 59/98 (60.2%, STE) vs. n = 47/98(48.0%,非STE, p = 0.115);n = 39/98 (39.8%, STE)与n = 27/98 (27.6%, non-STE; p = 0.096)为房车。在第7天以非STE标准评估时,更多的患者从SIMD中恢复(35.3% vs. 17.5% STE, p = 0.033),但在第30天没有(24.5% vs. 18.8% STE, p = 0.501)。30天死亡率(n = 33/ 98,33.7%)与非STE诊断的SIMD相关(p = 0.010),但与STE无关(p = 0.057)。在Cox回归中,只有非ste标准的LVDD预测30天死亡率(p = 0.005)。结论:采用STE标准时脓毒性休克中SIMD的发生率较高,且第一周可逆性较低。使用STE标准对SIMD的广义定义似乎没有提供额外的预后价值。试验注册:ClinicalTrials.gov: NCT05552521,于2022年9月20日注册。
Sepsis-induced myocardial dysfunction diagnosed with strain versus non-strain echocardiography parameters: incidence, evolution and association with prognosis.
Background: Sepsis-induced myocardial dysfunction (SIMD) remains poorly defined due to scarce longitudinal studies with advanced echocardiography. We characterized SIMD progression using speckle tracking echocardiography (STE).
Methods: Prospective single-center study in septic shock patients admitted to intensive care. SIMD was defined as any left ventricular (LV, systolic and/or diastolic) and/or right ventricular (RV) systolic dysfunction, using STE or non-STE criteria, on days 1, 7 and 30. We studied prevalence, evolution and prognosis of SIMD classified with either criteria using Cox regression.
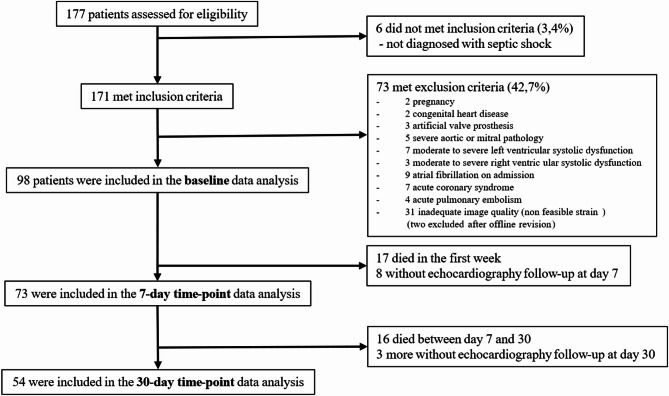
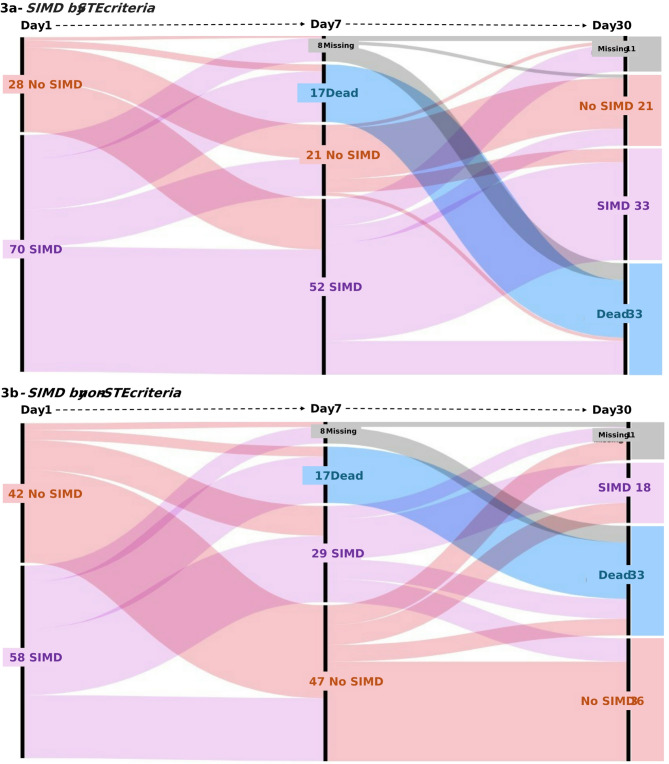
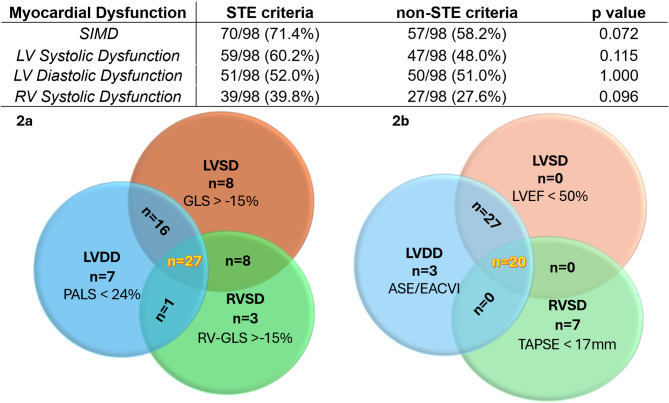
Results: Ninety-eight consecutive patients were included. On day 1, SIMD was identified in n = 57/98 (58.2%) and n = 70/98 (71.4%;p = 0.072) by non-STE and STE parameters, respectively. No significant difference in diagnosis was seen for LV diastolic dysfunction: n = 50/98 (51.0%, non-STE) vs. n = 51/98 (52.0%, STE; p = 1.00). Prevalences of LV and RV systolic dysfunction were not significantly higher with STE criteria: n = 59/98 (60.2%, STE) vs. n = 47/98 (48.0%, non-STE; p = 0.115) for LV; n = 39/98 (39.8%, STE) vs. n = 27/98 (27.6%, non-STE; p = 0.096) for RV. More patients recovered from SIMD when evaluated with non-STE criteria at day 7 (35.3% vs. 17.5% STE; p = 0.033), but not at day 30 (24.5% vs. 18.8% STE; p = 0.501). The 30-day mortality (n = 33/98, 33.7%) was associated with SIMD diagnosed using non-STE (p = 0.010), but not with STE (p = 0.057). In Cox regression, only LVDD by non-STE criteria predicted 30-day mortality (p = 0.005).
Conclusions: The incidence of SIMD in septic shock is higher when using STE criteria, with lower reversibility in the first week. A broad definition of SIMD utilizing STE criteria does not seem to provide additional prognostic value.
Trial registration: ClinicalTrials.gov: NCT05552521 registered on the 20th of September 2022.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


