Adam Muhammad Reid, Sarathi Bhattacharyya, Zian Zhuang, Nida Qadir, Amy Schnabel, Alan Chiem, Semi Yoon, George Lim, Igor Barjaktarevic
{"title":"在机械通气、营养不良、终末期肝病移植前患者中,膜片作为拔管成功的预测因素的即时超声评价——观察队列研究","authors":"Adam Muhammad Reid, Sarathi Bhattacharyya, Zian Zhuang, Nida Qadir, Amy Schnabel, Alan Chiem, Semi Yoon, George Lim, Igor Barjaktarevic","doi":"10.1177/29768675251337833","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ultrasound evaluation of diaphragmatic anatomy and function has recently gained traction as a simple and useful tool to assess the extubation readiness in mechanically ventilated patients, nevertheless, how applicable this approach is in the population of chronically debilitated patients on mechanical ventilation (MV) remains unclear.</p><p><strong>Objective: </strong>To evaluate ultrasonographic assessment of diaphragmatic thickening fraction (ΔTDI%) as a predictor of extubation success in the population of end-stage liver disease (ESLD) malnourished patients on MV.</p><p><strong>Design: </strong>Prospective, single-center, observational cohort study.</p><p><strong>Methods: </strong>We used point-of-care ultrasound to evaluate ΔTDI% and diaphragm thickness during expiration (<i>T</i> <sub>exp</sub>) and inspiration (<i>T</i> <sub>insp</sub>) as predictors of extubation success in ESLD patients undergoing weaning from mechanical ventilation. The primary end-point was extubation tolerance (ET) assessed at 48 h.</p><p><strong>Results: </strong>Of 70 enrolled patients, 82.4% (<i>N</i> = 56) tolerated extubation. While there was no difference in ΔTDI% between those who failed extubation (EF) compared to ET at 48 h (21.2% vs 20.1%, <i>P</i> = .64), diaphragms were thicker at expiration in ET patients (<i>T</i> <sub>exp</sub> 29.5 ± 8.1 vs 24.8 ± 5.2 mm, <i>P</i> = .047). Commonly used clinical weaning parameters, including rapid-shallow breathing index (RSBI) and negative inspiratory force (NIF) correlated better with diaphragm thickening fraction ΔTDI% than diaphragm thickness indices but were inferior predictors of extubation success compared to <i>T</i> <sub>exp.</sub>.</p><p><strong>Conclusion: </strong>Point-of-care ultrasonographic assessment of the diaphragm offers insight into the function of respiratory muscles and the limited ability to predict extubation success. Further research is necessary to better understand its potential use in MV liberation in patients with ESLD and malnutrition.</p>","PeriodicalId":94361,"journal":{"name":"Therapeutic advances in pulmonary and critical care medicine","volume":"20 ","pages":"29768675251337833"},"PeriodicalIF":3.0000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12451113/pdf/","citationCount":"0","resultStr":"{\"title\":\"Point-of-Care Ultrasound Evaluation of Diaphragm as a Predictor of Extubation Success in Mechanically Ventilated, Malnourished, End-Stage Liver Disease Pretransplant Candidates-Observational Cohort Study.\",\"authors\":\"Adam Muhammad Reid, Sarathi Bhattacharyya, Zian Zhuang, Nida Qadir, Amy Schnabel, Alan Chiem, Semi Yoon, George Lim, Igor Barjaktarevic\",\"doi\":\"10.1177/29768675251337833\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Ultrasound evaluation of diaphragmatic anatomy and function has recently gained traction as a simple and useful tool to assess the extubation readiness in mechanically ventilated patients, nevertheless, how applicable this approach is in the population of chronically debilitated patients on mechanical ventilation (MV) remains unclear.</p><p><strong>Objective: </strong>To evaluate ultrasonographic assessment of diaphragmatic thickening fraction (ΔTDI%) as a predictor of extubation success in the population of end-stage liver disease (ESLD) malnourished patients on MV.</p><p><strong>Design: </strong>Prospective, single-center, observational cohort study.</p><p><strong>Methods: </strong>We used point-of-care ultrasound to evaluate ΔTDI% and diaphragm thickness during expiration (<i>T</i> <sub>exp</sub>) and inspiration (<i>T</i> <sub>insp</sub>) as predictors of extubation success in ESLD patients undergoing weaning from mechanical ventilation. The primary end-point was extubation tolerance (ET) assessed at 48 h.</p><p><strong>Results: </strong>Of 70 enrolled patients, 82.4% (<i>N</i> = 56) tolerated extubation. While there was no difference in ΔTDI% between those who failed extubation (EF) compared to ET at 48 h (21.2% vs 20.1%, <i>P</i> = .64), diaphragms were thicker at expiration in ET patients (<i>T</i> <sub>exp</sub> 29.5 ± 8.1 vs 24.8 ± 5.2 mm, <i>P</i> = .047). Commonly used clinical weaning parameters, including rapid-shallow breathing index (RSBI) and negative inspiratory force (NIF) correlated better with diaphragm thickening fraction ΔTDI% than diaphragm thickness indices but were inferior predictors of extubation success compared to <i>T</i> <sub>exp.</sub>.</p><p><strong>Conclusion: </strong>Point-of-care ultrasonographic assessment of the diaphragm offers insight into the function of respiratory muscles and the limited ability to predict extubation success. Further research is necessary to better understand its potential use in MV liberation in patients with ESLD and malnutrition.</p>\",\"PeriodicalId\":94361,\"journal\":{\"name\":\"Therapeutic advances in pulmonary and critical care medicine\",\"volume\":\"20 \",\"pages\":\"29768675251337833\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12451113/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic advances in pulmonary and critical care medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/29768675251337833\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"0\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic advances in pulmonary and critical care medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/29768675251337833","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"0","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
背景:超声评估膈解剖和功能作为一种简单而有用的工具,用于评估机械通气患者拔管准备情况,最近得到了广泛的关注,然而,这种方法在机械通气(MV)慢性衰弱患者群体中的适用性尚不清楚。目的:评价超声评价膈增厚分数(ΔTDI%)作为终末期肝病(ESLD)营养不良患者MV拔管成功率的预测指标。设计:前瞻性、单中心、观察队列研究。方法:我们使用护理点超声评估ΔTDI%和呼气时隔膜厚度(T exp)和吸气时隔膜厚度(T insp)作为ESLD患者脱离机械通气拔管成功的预测因素。主要终点是在48小时评估拔管耐受性(ET)。结果:70例入组患者中,82.4% (N = 56)患者耐受拔管。而拔管失败(EF)组与ET组在48 h时的ΔTDI%无差异(21.2% vs 20.1%, P =。ET患者呼气时膈膜较厚(T exp 29.5±8.1 vs 24.8±5.2 mm, P = 0.047)。常用的临床脱机参数,包括快速浅呼吸指数(RSBI)和负吸气力(NIF)与隔膜增厚分数ΔTDI%的相关性优于隔膜厚度指数,但与T exp相比,它们是拔管成功的较差预测指标。结论:对隔膜的即时超声评估有助于了解呼吸肌的功能和预测拔管成功的有限能力。需要进一步的研究来更好地了解其在ESLD和营养不良患者的MV释放中的潜在应用。
Point-of-Care Ultrasound Evaluation of Diaphragm as a Predictor of Extubation Success in Mechanically Ventilated, Malnourished, End-Stage Liver Disease Pretransplant Candidates-Observational Cohort Study.
Background: Ultrasound evaluation of diaphragmatic anatomy and function has recently gained traction as a simple and useful tool to assess the extubation readiness in mechanically ventilated patients, nevertheless, how applicable this approach is in the population of chronically debilitated patients on mechanical ventilation (MV) remains unclear.
Objective: To evaluate ultrasonographic assessment of diaphragmatic thickening fraction (ΔTDI%) as a predictor of extubation success in the population of end-stage liver disease (ESLD) malnourished patients on MV.
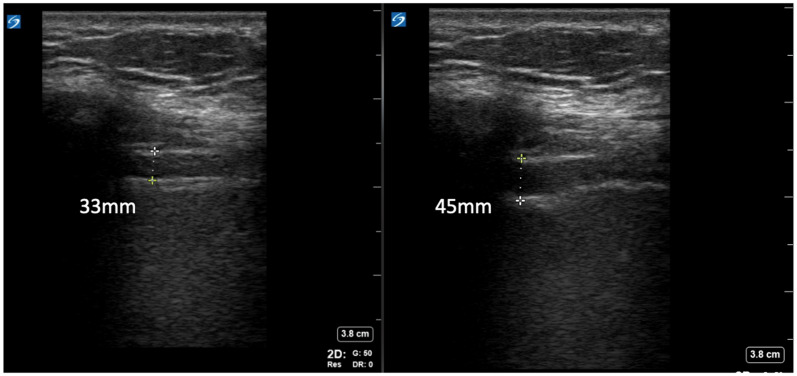
Methods: We used point-of-care ultrasound to evaluate ΔTDI% and diaphragm thickness during expiration (Texp) and inspiration (Tinsp) as predictors of extubation success in ESLD patients undergoing weaning from mechanical ventilation. The primary end-point was extubation tolerance (ET) assessed at 48 h.
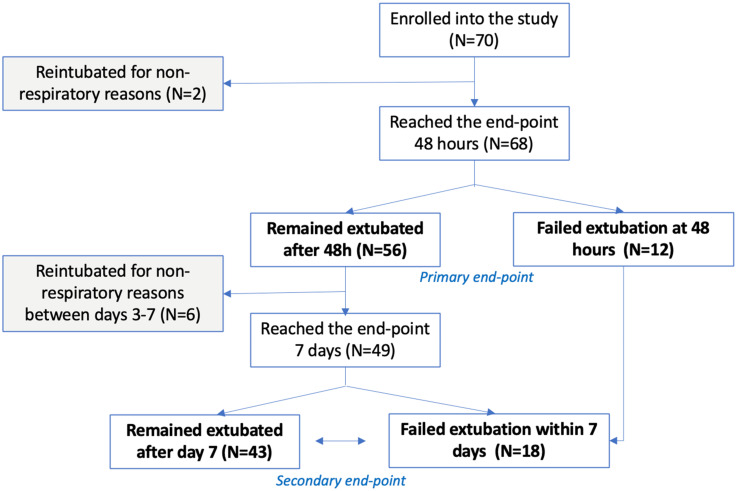
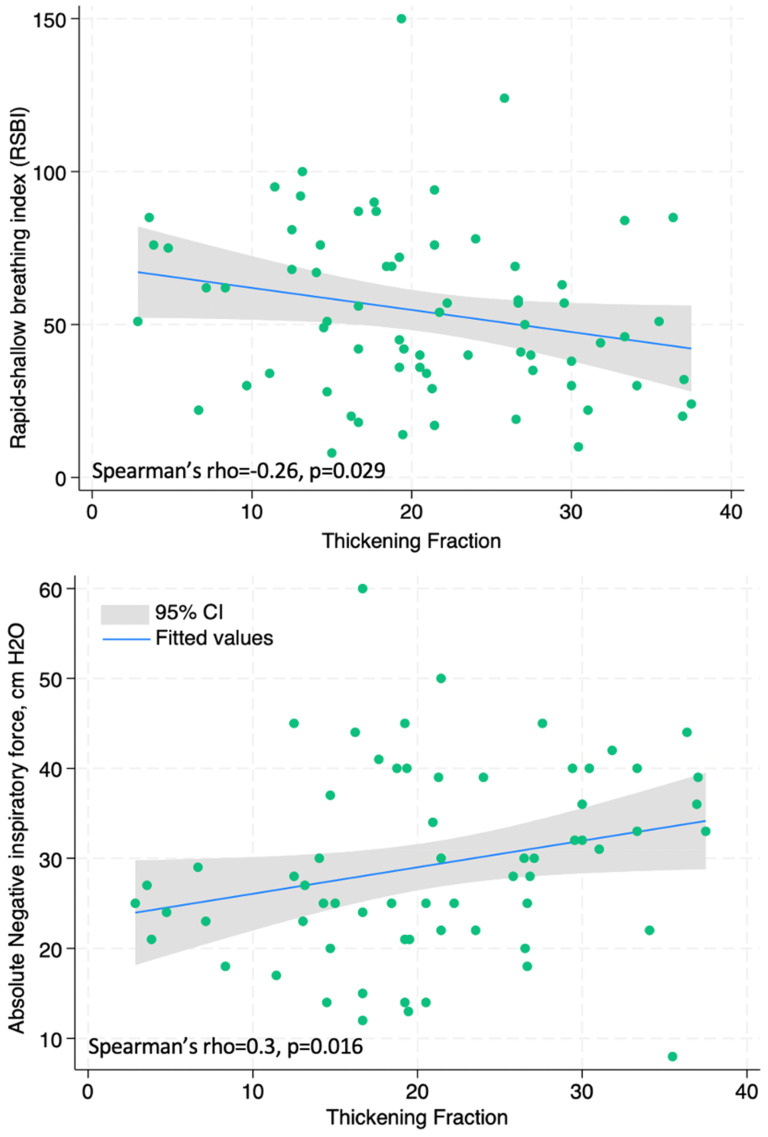
Results: Of 70 enrolled patients, 82.4% (N = 56) tolerated extubation. While there was no difference in ΔTDI% between those who failed extubation (EF) compared to ET at 48 h (21.2% vs 20.1%, P = .64), diaphragms were thicker at expiration in ET patients (Texp 29.5 ± 8.1 vs 24.8 ± 5.2 mm, P = .047). Commonly used clinical weaning parameters, including rapid-shallow breathing index (RSBI) and negative inspiratory force (NIF) correlated better with diaphragm thickening fraction ΔTDI% than diaphragm thickness indices but were inferior predictors of extubation success compared to Texp..
Conclusion: Point-of-care ultrasonographic assessment of the diaphragm offers insight into the function of respiratory muscles and the limited ability to predict extubation success. Further research is necessary to better understand its potential use in MV liberation in patients with ESLD and malnutrition.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


