Cassandra Sundaraja, Suzanne M Cosh, Amy Dianne Lykins, Hayley Farrell, Hira Masood, Melanie Kelly Williams, Jyoti Chaku, Joseph Turner, Anand Swamy, Phillip J Tully
{"title":"基于群体的分娩创伤远程医疗干预:试点可行性和候补控制试验方案。","authors":"Cassandra Sundaraja, Suzanne M Cosh, Amy Dianne Lykins, Hayley Farrell, Hira Masood, Melanie Kelly Williams, Jyoti Chaku, Joseph Turner, Anand Swamy, Phillip J Tully","doi":"10.2196/69051","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Traumatic childbirth experiences affect almost half of Australian women giving birth and can lead to significant mental health impacts, including postpartum depression, anxiety. and posttraumatic stress disorder (PTSD). Despite evidence supporting psychological interventions for birth trauma, there are prominent gaps in the accessibility of these treatments, particularly for postpartum women in regional or rural areas, who face long waitlists, geographical isolation, and high financial costs. Although narrative approaches hold promise for addressing birth-related trauma, no research study to date has specifically trialed a narrative-informed, group-based telehealth intervention in this space.</p><p><strong>Objective: </strong>This study aims to assess the acceptability and feasibility of a narrative-informed, group-based telehealth intervention for postpartum women in reducing the mental health impacts of having experienced a traumatic childbirth.</p><p><strong>Methods: </strong>This pilot feasibility trial with a waitlist control design evaluated a six-session narrative-informed, group-based intervention delivered weekly via telehealth to postpartum women who experienced a traumatic childbirth within the past 6 months. The intervention incorporated narrative therapy techniques, such as externalization, double-listening, and outsider witnessing. Participants from a specific catchment area of predominantly rural towns in New South Wales in Australia were randomly assigned to either an intervention group (IG) or a waitlist control group (WCG). Quantitative measures assessing mental health symptoms of postpartum depression (Edinburgh Postnatal Depression Scale [EPDS]), anxiety (Perinatal Anxiety Screening Scale [PASS]) and posttraumatic stress (City Birth Trauma Scale [City BiTS]) were administered prior to, in between, and at the end of treatment, and measures of client satisfaction (Client Satisfaction Questionnaire [CSQ-8]) and group cohesion (Group Cohesiveness Scale [GCS]) were administered on completion of the intervention.</p><p><strong>Results: </strong>The project was funded in March 2024. Recruitment was completed between July and August 2024. Eleven pretreatment sessions were held in August 2024. Of the 33 expressions of interest (EOIs) received by August 2024, 9 participants were recruited and randomized to the IG (n=4, 44.4%) and the WCG (n=5, 55.6%). The IG completed the six-session program between September and October 2024, with data collection finalized for pre-, mid-, and postintervention timepoints. The WCG began receiving the intervention mid-October 2024, with the final data collection in December 2024. Key feasibility and acceptability metrics include attendance rates, participant retention, and group cohesion scores. Data analysis is ongoing, with manuscript preparation planned for mid-late 2025.</p><p><strong>Conclusions: </strong>This study addresses a critical gap in evaluating scalable, accessible mental health interventions for birth trauma recovery. By using narrative approaches in a telehealth group format, this intervention directly responds to the barriers around accessibility and affordability highlighted in recent policy recommendations. Thus, findings from this pilot study could provide important directions in reducing the burden on perinatal mental health services in regional and rural Australia.</p><p><strong>Trial registration: </strong>Australian New Zealand Clinical Trials Registry ANZCTR12624000460505p; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12624000460505p.</p><p><strong>International registered report identifier (irrid): </strong>DERR1-10.2196/69051.</p>","PeriodicalId":14755,"journal":{"name":"JMIR Research Protocols","volume":"14 ","pages":"e69051"},"PeriodicalIF":1.5000,"publicationDate":"2025-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12504894/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Group-Based Telehealth Intervention for Birth Trauma: Protocol for a Pilot Feasibility and Waitlist Control Trial.\",\"authors\":\"Cassandra Sundaraja, Suzanne M Cosh, Amy Dianne Lykins, Hayley Farrell, Hira Masood, Melanie Kelly Williams, Jyoti Chaku, Joseph Turner, Anand Swamy, Phillip J Tully\",\"doi\":\"10.2196/69051\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Traumatic childbirth experiences affect almost half of Australian women giving birth and can lead to significant mental health impacts, including postpartum depression, anxiety. and posttraumatic stress disorder (PTSD). Despite evidence supporting psychological interventions for birth trauma, there are prominent gaps in the accessibility of these treatments, particularly for postpartum women in regional or rural areas, who face long waitlists, geographical isolation, and high financial costs. Although narrative approaches hold promise for addressing birth-related trauma, no research study to date has specifically trialed a narrative-informed, group-based telehealth intervention in this space.</p><p><strong>Objective: </strong>This study aims to assess the acceptability and feasibility of a narrative-informed, group-based telehealth intervention for postpartum women in reducing the mental health impacts of having experienced a traumatic childbirth.</p><p><strong>Methods: </strong>This pilot feasibility trial with a waitlist control design evaluated a six-session narrative-informed, group-based intervention delivered weekly via telehealth to postpartum women who experienced a traumatic childbirth within the past 6 months. The intervention incorporated narrative therapy techniques, such as externalization, double-listening, and outsider witnessing. Participants from a specific catchment area of predominantly rural towns in New South Wales in Australia were randomly assigned to either an intervention group (IG) or a waitlist control group (WCG). Quantitative measures assessing mental health symptoms of postpartum depression (Edinburgh Postnatal Depression Scale [EPDS]), anxiety (Perinatal Anxiety Screening Scale [PASS]) and posttraumatic stress (City Birth Trauma Scale [City BiTS]) were administered prior to, in between, and at the end of treatment, and measures of client satisfaction (Client Satisfaction Questionnaire [CSQ-8]) and group cohesion (Group Cohesiveness Scale [GCS]) were administered on completion of the intervention.</p><p><strong>Results: </strong>The project was funded in March 2024. Recruitment was completed between July and August 2024. Eleven pretreatment sessions were held in August 2024. Of the 33 expressions of interest (EOIs) received by August 2024, 9 participants were recruited and randomized to the IG (n=4, 44.4%) and the WCG (n=5, 55.6%). The IG completed the six-session program between September and October 2024, with data collection finalized for pre-, mid-, and postintervention timepoints. The WCG began receiving the intervention mid-October 2024, with the final data collection in December 2024. Key feasibility and acceptability metrics include attendance rates, participant retention, and group cohesion scores. Data analysis is ongoing, with manuscript preparation planned for mid-late 2025.</p><p><strong>Conclusions: </strong>This study addresses a critical gap in evaluating scalable, accessible mental health interventions for birth trauma recovery. By using narrative approaches in a telehealth group format, this intervention directly responds to the barriers around accessibility and affordability highlighted in recent policy recommendations. Thus, findings from this pilot study could provide important directions in reducing the burden on perinatal mental health services in regional and rural Australia.</p><p><strong>Trial registration: </strong>Australian New Zealand Clinical Trials Registry ANZCTR12624000460505p; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12624000460505p.</p><p><strong>International registered report identifier (irrid): </strong>DERR1-10.2196/69051.</p>\",\"PeriodicalId\":14755,\"journal\":{\"name\":\"JMIR Research Protocols\",\"volume\":\"14 \",\"pages\":\"e69051\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12504894/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR Research Protocols\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/69051\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Research Protocols","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/69051","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
A Group-Based Telehealth Intervention for Birth Trauma: Protocol for a Pilot Feasibility and Waitlist Control Trial.
Background: Traumatic childbirth experiences affect almost half of Australian women giving birth and can lead to significant mental health impacts, including postpartum depression, anxiety. and posttraumatic stress disorder (PTSD). Despite evidence supporting psychological interventions for birth trauma, there are prominent gaps in the accessibility of these treatments, particularly for postpartum women in regional or rural areas, who face long waitlists, geographical isolation, and high financial costs. Although narrative approaches hold promise for addressing birth-related trauma, no research study to date has specifically trialed a narrative-informed, group-based telehealth intervention in this space.
Objective: This study aims to assess the acceptability and feasibility of a narrative-informed, group-based telehealth intervention for postpartum women in reducing the mental health impacts of having experienced a traumatic childbirth.
Methods: This pilot feasibility trial with a waitlist control design evaluated a six-session narrative-informed, group-based intervention delivered weekly via telehealth to postpartum women who experienced a traumatic childbirth within the past 6 months. The intervention incorporated narrative therapy techniques, such as externalization, double-listening, and outsider witnessing. Participants from a specific catchment area of predominantly rural towns in New South Wales in Australia were randomly assigned to either an intervention group (IG) or a waitlist control group (WCG). Quantitative measures assessing mental health symptoms of postpartum depression (Edinburgh Postnatal Depression Scale [EPDS]), anxiety (Perinatal Anxiety Screening Scale [PASS]) and posttraumatic stress (City Birth Trauma Scale [City BiTS]) were administered prior to, in between, and at the end of treatment, and measures of client satisfaction (Client Satisfaction Questionnaire [CSQ-8]) and group cohesion (Group Cohesiveness Scale [GCS]) were administered on completion of the intervention.
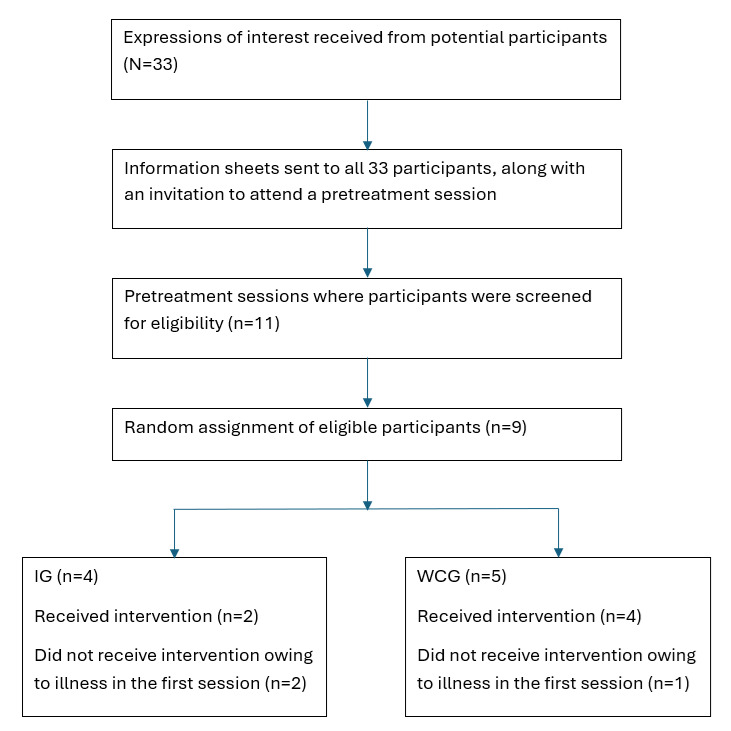
Results: The project was funded in March 2024. Recruitment was completed between July and August 2024. Eleven pretreatment sessions were held in August 2024. Of the 33 expressions of interest (EOIs) received by August 2024, 9 participants were recruited and randomized to the IG (n=4, 44.4%) and the WCG (n=5, 55.6%). The IG completed the six-session program between September and October 2024, with data collection finalized for pre-, mid-, and postintervention timepoints. The WCG began receiving the intervention mid-October 2024, with the final data collection in December 2024. Key feasibility and acceptability metrics include attendance rates, participant retention, and group cohesion scores. Data analysis is ongoing, with manuscript preparation planned for mid-late 2025.
Conclusions: This study addresses a critical gap in evaluating scalable, accessible mental health interventions for birth trauma recovery. By using narrative approaches in a telehealth group format, this intervention directly responds to the barriers around accessibility and affordability highlighted in recent policy recommendations. Thus, findings from this pilot study could provide important directions in reducing the burden on perinatal mental health services in regional and rural Australia.
Trial registration: Australian New Zealand Clinical Trials Registry ANZCTR12624000460505p; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12624000460505p.
International registered report identifier (irrid): DERR1-10.2196/69051.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


