Dalton McLean, John Rommel, John A Steuter, William S Carroll, Mark Rabbat, Sudarshan Rajagopal, Venkatraman Srinivasan, Dean J Kereiakes, Michael C Roberts, Abhijit Raval, Navid Nemati, Farhad Fathieh, Timothy Burton, Horace R Gillins, Ian Shadforth, Shyam Ramchandani, Charles R Bridges, Vallerie V McLaughlin
{"title":"识别肺动脉高压的机器学习即时护理系统的临床验证。","authors":"Dalton McLean, John Rommel, John A Steuter, William S Carroll, Mark Rabbat, Sudarshan Rajagopal, Venkatraman Srinivasan, Dean J Kereiakes, Michael C Roberts, Abhijit Raval, Navid Nemati, Farhad Fathieh, Timothy Burton, Horace R Gillins, Ian Shadforth, Shyam Ramchandani, Charles R Bridges, Vallerie V McLaughlin","doi":"10.1183/23120541.01287-2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pulmonary hypertension (PH) is a collection of diverse disorders, defined by mean pulmonary artery pressure (mPAP) ≥21 mmHg (most recent guidelines) or ≥25 mmHg (previous guidelines, that underpins the field's past work) measured by right heart catheterisation (RHC). Considering the difficulties in diagnosing PH and the subsequent treatment delays, there is a need for novel diagnostics to enable prompt detection.</p><p><strong>Methods: </strong>An algorithm to assess mPAP elevation was validated using subjects with elevated mPAP from RHC (positive cohort) and subjects with low probability of PH by stringent screening of transthoracic echocardiography (TTE) PH indicators (negative cohort). 25 mmHg and 21 mmHg were pre-specified as the co-primary and secondary sensitivity end-points, respectively, at 0.70. Specificity was the co-primary end-point at 0.60. The algorithm cut-point was pre-defined. The area under the receiver operator characteristic curve (ROC-AUC) was assessed at both mPAP thresholds.</p><p><strong>Findings: </strong>462 subjects were consecutively enrolled across 18 US clinical sites between August 2019 and September 2022. Sensitivity at 25 mmHg and 21 mmHg was 0.82 (95% CI 0.78-0.87) and 0.78 (95% CI 0.73-0.82), respectively, with specificity of 0.92 (95% CI 0.87-0.96), passing the study end-points. The ROC-AUC values at 25 mmHg and 21 mmHg were 0.95 (95% CI 0.93-0.96) and 0.93 (95% CI 0.91-0.95), respectively. Further, performance was similar across PH subgroups (pre-capillary, combined pre- and post-capillary, and isolated post-capillary), as well as between men and women.</p><p><strong>Interpretation: </strong>The algorithm's performance is comparable, or possibly superior to, TTE, given that the tricuspid regurgitant velocity is not measurable in up to 41% of TTE cases. The test is a stress-free, noninvasive front-line test, presenting advantages to patients, physicians and healthcare systems.</p>","PeriodicalId":11739,"journal":{"name":"ERJ Open Research","volume":"11 5","pages":""},"PeriodicalIF":4.0000,"publicationDate":"2025-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12451580/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical validation of a machine-learned, point-of-care system to IDENTIFY pulmonary hypertension.\",\"authors\":\"Dalton McLean, John Rommel, John A Steuter, William S Carroll, Mark Rabbat, Sudarshan Rajagopal, Venkatraman Srinivasan, Dean J Kereiakes, Michael C Roberts, Abhijit Raval, Navid Nemati, Farhad Fathieh, Timothy Burton, Horace R Gillins, Ian Shadforth, Shyam Ramchandani, Charles R Bridges, Vallerie V McLaughlin\",\"doi\":\"10.1183/23120541.01287-2024\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Pulmonary hypertension (PH) is a collection of diverse disorders, defined by mean pulmonary artery pressure (mPAP) ≥21 mmHg (most recent guidelines) or ≥25 mmHg (previous guidelines, that underpins the field's past work) measured by right heart catheterisation (RHC). Considering the difficulties in diagnosing PH and the subsequent treatment delays, there is a need for novel diagnostics to enable prompt detection.</p><p><strong>Methods: </strong>An algorithm to assess mPAP elevation was validated using subjects with elevated mPAP from RHC (positive cohort) and subjects with low probability of PH by stringent screening of transthoracic echocardiography (TTE) PH indicators (negative cohort). 25 mmHg and 21 mmHg were pre-specified as the co-primary and secondary sensitivity end-points, respectively, at 0.70. Specificity was the co-primary end-point at 0.60. The algorithm cut-point was pre-defined. The area under the receiver operator characteristic curve (ROC-AUC) was assessed at both mPAP thresholds.</p><p><strong>Findings: </strong>462 subjects were consecutively enrolled across 18 US clinical sites between August 2019 and September 2022. Sensitivity at 25 mmHg and 21 mmHg was 0.82 (95% CI 0.78-0.87) and 0.78 (95% CI 0.73-0.82), respectively, with specificity of 0.92 (95% CI 0.87-0.96), passing the study end-points. The ROC-AUC values at 25 mmHg and 21 mmHg were 0.95 (95% CI 0.93-0.96) and 0.93 (95% CI 0.91-0.95), respectively. Further, performance was similar across PH subgroups (pre-capillary, combined pre- and post-capillary, and isolated post-capillary), as well as between men and women.</p><p><strong>Interpretation: </strong>The algorithm's performance is comparable, or possibly superior to, TTE, given that the tricuspid regurgitant velocity is not measurable in up to 41% of TTE cases. The test is a stress-free, noninvasive front-line test, presenting advantages to patients, physicians and healthcare systems.</p>\",\"PeriodicalId\":11739,\"journal\":{\"name\":\"ERJ Open Research\",\"volume\":\"11 5\",\"pages\":\"\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2025-09-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12451580/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ERJ Open Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1183/23120541.01287-2024\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ERJ Open Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1183/23120541.01287-2024","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
背景:肺动脉高压(PH)是多种疾病的集合,通过右心导管(RHC)测量的平均肺动脉压(mPAP)≥21 mmHg(最新指南)或≥25 mmHg(以前的指南,支持该领域过去的工作)来定义。考虑到诊断PH的困难和随后的治疗延误,需要新的诊断方法来实现及时检测。方法:通过严格筛选经胸超声心动图(TTE) PH指标(阴性队列),对RHC中mPAP升高的受试者(阳性队列)和PH低概率的受试者(阴性队列)进行mPAP升高评估的算法进行验证。25 mmHg和21 mmHg被预先指定为主要和次要敏感性终点,分别为0.70。特异性是共同主要终点,为0.60。算法截断点是预先定义的。在两个mPAP阈值下评估受试者操作者特征曲线下的面积(ROC-AUC)。研究结果:2019年8月至2022年9月期间,462名受试者在美国18个临床站点连续入组。25 mmHg和21 mmHg时的敏感性分别为0.82 (95% CI 0.78-0.87)和0.78 (95% CI 0.73-0.82),特异性为0.92 (95% CI 0.87-0.96),通过了研究终点。25 mmHg和21 mmHg时ROC-AUC值分别为0.95 (95% CI 0.93-0.96)和0.93 (95% CI 0.91-0.95)。此外,PH亚组(毛细血管前、联合毛细血管前后和分离毛细血管后)以及男性和女性之间的表现相似。解释:该算法的性能与TTE相当,甚至可能优于TTE,因为在高达41%的TTE病例中,三尖瓣反流速度无法测量。该测试是一种无压力、无创的一线测试,对患者、医生和医疗保健系统都有好处。
Clinical validation of a machine-learned, point-of-care system to IDENTIFY pulmonary hypertension.
Background: Pulmonary hypertension (PH) is a collection of diverse disorders, defined by mean pulmonary artery pressure (mPAP) ≥21 mmHg (most recent guidelines) or ≥25 mmHg (previous guidelines, that underpins the field's past work) measured by right heart catheterisation (RHC). Considering the difficulties in diagnosing PH and the subsequent treatment delays, there is a need for novel diagnostics to enable prompt detection.
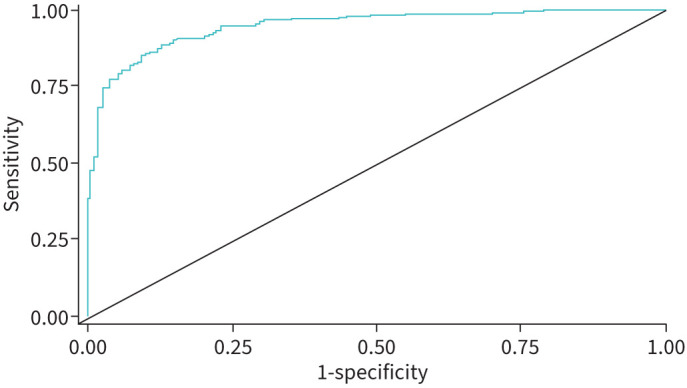
Methods: An algorithm to assess mPAP elevation was validated using subjects with elevated mPAP from RHC (positive cohort) and subjects with low probability of PH by stringent screening of transthoracic echocardiography (TTE) PH indicators (negative cohort). 25 mmHg and 21 mmHg were pre-specified as the co-primary and secondary sensitivity end-points, respectively, at 0.70. Specificity was the co-primary end-point at 0.60. The algorithm cut-point was pre-defined. The area under the receiver operator characteristic curve (ROC-AUC) was assessed at both mPAP thresholds.
Findings: 462 subjects were consecutively enrolled across 18 US clinical sites between August 2019 and September 2022. Sensitivity at 25 mmHg and 21 mmHg was 0.82 (95% CI 0.78-0.87) and 0.78 (95% CI 0.73-0.82), respectively, with specificity of 0.92 (95% CI 0.87-0.96), passing the study end-points. The ROC-AUC values at 25 mmHg and 21 mmHg were 0.95 (95% CI 0.93-0.96) and 0.93 (95% CI 0.91-0.95), respectively. Further, performance was similar across PH subgroups (pre-capillary, combined pre- and post-capillary, and isolated post-capillary), as well as between men and women.
Interpretation: The algorithm's performance is comparable, or possibly superior to, TTE, given that the tricuspid regurgitant velocity is not measurable in up to 41% of TTE cases. The test is a stress-free, noninvasive front-line test, presenting advantages to patients, physicians and healthcare systems.
期刊介绍:
ERJ Open Research is a fully open access original research journal, published online by the European Respiratory Society. The journal aims to publish high-quality work in all fields of respiratory science and medicine, covering basic science, clinical translational science and clinical medicine. The journal was created to help fulfil the ERS objective to disseminate scientific and educational material to its members and to the medical community, but also to provide researchers with an affordable open access specialty journal in which to publish their work.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


