Yangming Cao, Thao Phan, Patil Armenian, Jonathan E Zuckerman
{"title":"引起急性肾损伤和肾病综合征的“神奇药丸”。","authors":"Yangming Cao, Thao Phan, Patil Armenian, Jonathan E Zuckerman","doi":"10.5414/CNCS111804","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The sudden onset of nephrotic syndrome (NS) and acute interstitial nephritis (AIN) seems to be an uncommon but distinct nonsteroidal anti-inflammatory drug (NSAID)-related renal syndrome.</p><p><strong>Case presentation: </strong>We present such a case in a patient who took a \"magic pill\" for gout. Renal biopsy revealed minimal change disease (MCD), acute interstitial nephritis (AIN), severe acute tubular injury (ATI), and IgA nephropathy (IgAN). He was treated with an aborted course of high-dose prednisone, with complete resolution of his renal diseases. The pathologic finding of the combination of MCD and AIN raised the possibility of a drug effect. One of the pills was analyzed and found to be primarily composed of diclofenac. Initially, we considered IgAN a bystander, considering primary IgAN is the most common glomerulonephritis worldwide, especially in Asians and Hispanics. However, the complete resolution of urinary findings after discontinuation of the pill followed by a few days' treatment with prednisone, together with no recurrence of the kidney disease over 6 years, made us speculate that IgAN may have also been triggered by diclofenac.</p><p><strong>Conclusion: </strong>We presented a case of AIN, MCD, and IgAN associated with diclofenac masquerading as a \"herbal\" medicine. The cause was suggested by pathology and confirmed with high-resolution liquid chromatography mass spectrometry testing of the pills. A history of NSAID use should be diligently sought in any patient who presents with NS and AIN. In addition, this is the first report of IgAN possibly induced by NSAID without recurrence after 6 years' follow-up.</p>","PeriodicalId":510898,"journal":{"name":"Clinical nephrology. Case studies","volume":"13 ","pages":"59-65"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12444431/pdf/","citationCount":"0","resultStr":"{\"title\":\"Acute kidney injury and nephrotic syndrome caused by a \\\"magic pill\\\".\",\"authors\":\"Yangming Cao, Thao Phan, Patil Armenian, Jonathan E Zuckerman\",\"doi\":\"10.5414/CNCS111804\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The sudden onset of nephrotic syndrome (NS) and acute interstitial nephritis (AIN) seems to be an uncommon but distinct nonsteroidal anti-inflammatory drug (NSAID)-related renal syndrome.</p><p><strong>Case presentation: </strong>We present such a case in a patient who took a \\\"magic pill\\\" for gout. Renal biopsy revealed minimal change disease (MCD), acute interstitial nephritis (AIN), severe acute tubular injury (ATI), and IgA nephropathy (IgAN). He was treated with an aborted course of high-dose prednisone, with complete resolution of his renal diseases. The pathologic finding of the combination of MCD and AIN raised the possibility of a drug effect. One of the pills was analyzed and found to be primarily composed of diclofenac. Initially, we considered IgAN a bystander, considering primary IgAN is the most common glomerulonephritis worldwide, especially in Asians and Hispanics. However, the complete resolution of urinary findings after discontinuation of the pill followed by a few days' treatment with prednisone, together with no recurrence of the kidney disease over 6 years, made us speculate that IgAN may have also been triggered by diclofenac.</p><p><strong>Conclusion: </strong>We presented a case of AIN, MCD, and IgAN associated with diclofenac masquerading as a \\\"herbal\\\" medicine. The cause was suggested by pathology and confirmed with high-resolution liquid chromatography mass spectrometry testing of the pills. A history of NSAID use should be diligently sought in any patient who presents with NS and AIN. In addition, this is the first report of IgAN possibly induced by NSAID without recurrence after 6 years' follow-up.</p>\",\"PeriodicalId\":510898,\"journal\":{\"name\":\"Clinical nephrology. Case studies\",\"volume\":\"13 \",\"pages\":\"59-65\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12444431/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical nephrology. Case studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/CNCS111804\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical nephrology. Case studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS111804","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Acute kidney injury and nephrotic syndrome caused by a "magic pill".
Introduction: The sudden onset of nephrotic syndrome (NS) and acute interstitial nephritis (AIN) seems to be an uncommon but distinct nonsteroidal anti-inflammatory drug (NSAID)-related renal syndrome.
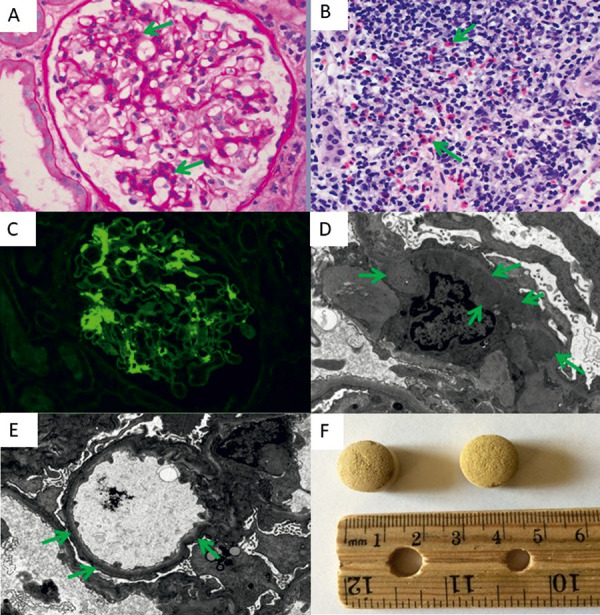
Case presentation: We present such a case in a patient who took a "magic pill" for gout. Renal biopsy revealed minimal change disease (MCD), acute interstitial nephritis (AIN), severe acute tubular injury (ATI), and IgA nephropathy (IgAN). He was treated with an aborted course of high-dose prednisone, with complete resolution of his renal diseases. The pathologic finding of the combination of MCD and AIN raised the possibility of a drug effect. One of the pills was analyzed and found to be primarily composed of diclofenac. Initially, we considered IgAN a bystander, considering primary IgAN is the most common glomerulonephritis worldwide, especially in Asians and Hispanics. However, the complete resolution of urinary findings after discontinuation of the pill followed by a few days' treatment with prednisone, together with no recurrence of the kidney disease over 6 years, made us speculate that IgAN may have also been triggered by diclofenac.
Conclusion: We presented a case of AIN, MCD, and IgAN associated with diclofenac masquerading as a "herbal" medicine. The cause was suggested by pathology and confirmed with high-resolution liquid chromatography mass spectrometry testing of the pills. A history of NSAID use should be diligently sought in any patient who presents with NS and AIN. In addition, this is the first report of IgAN possibly induced by NSAID without recurrence after 6 years' follow-up.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


