{"title":"甲状腺疾病妇女补充左旋甲状腺素与妊娠结局:随机对照试验的系统评价和荟萃分析综述","authors":"Jing Wang, Jiashu Li, Jing Zhang, Aihua Liu, Wanyu Yang, Xiaodan Zhai, Weiping Teng, Yongze Li, Zhongyan Shan","doi":"10.1093/hropen/hoaf036","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Does levothyroxine (LT4) treatment reduce adverse pregnancy outcomes in pregnant women with thyroid dysfunction?</p><p><strong>Summary answer: </strong>LT4 treatment significantly reduces the risks of pregnancy loss, preterm delivery, and gestational hypertension, with no significant impacts on rates of live birth, placental abruption, or gestational diabetes.</p><p><strong>What is known already: </strong>Multiple meta-analyses have examined the impact of LT4 on pregnancy outcomes, but quantitative confidence assessments are still lacking. Thus, an umbrella review is needed to systematically synthesize and assess the quality of this evidence.</p><p><strong>Study design size duration: </strong>This umbrella review of systematic reviews and meta-analyses used PubMed, Embase, Web of Science, and the Cochrane Database of Systematic Reviews. Searches included studies published in English or Chinese up to 20 March 2025.</p><p><strong>Participants/materials setting methods: </strong>Included studies were systematic reviews or meta-analyses of randomized controlled trials assessing the effects of LT4 on pregnancy outcomes in women with subclinical hypothyroidism (SCH) or thyroid peroxidase antibody (TPOAb) positivity. A set of 24 associations across six pregnancy outcomes were analyzed: pregnancy loss, preterm delivery, live birth, placental abruption, gestational hypertension, and gestational diabetes. Methodological quality was assessed using AMSTAR 1, and evidence quality was graded using GRADE. Sensitivity analyses were conducted to confirm robustness.</p><p><strong>Main results and the role of chance: </strong>Eleven meta-analyses were included. High-quality evidence showed that LT4 treatment reduced the risks of pregnancy loss (RR = 0.43; class III evidence), preterm delivery (RR = 0.56; class III evidence), and gestational hypertension (RR = 0.63; class IV evidence). Moderate-to-low-quality evidence indicated no significant impact on rates of live birth, placental abruption, or gestational diabetes. Of the 24 associations, 22 were rated as high confidence and two as medium confidence based on AMSTAR 1. Sensitivity analyses confirmed the robustness of the findings, but treatment effects varied according to the study population, treatment timing, and method. For pregnancy loss and preterm delivery outcomes, the risk was significantly reduced only when LT4 treatment was initiated in early pregnancy (pregnancy loss: RR = 0.60, <i>P</i> = 0.03; RR = 0.59, <i>P</i> = 0.003; preterm labor: RR = 0.58, <i>P </i>< 0.0001; RR = 0.46, <i>P</i> < 0.00001). Additionally, women with TSH levels greater than 4.0 mU/l derived greater benefits from LT4 treatment compared to those with TSH levels between 2.5 and 4.0 mU/l.</p><p><strong>Limitations reasons for caution: </strong>Limitations include small sample sizes, potential biases (selection and reporting), and language restrictions to English and Chinese studies, which may affect generalizability.</p><p><strong>Wider implications of the findings: </strong>By integrating high-quality evidence, this study confirms that LT4 can reduce the risk of pregnancy loss and preterm delivery in pregnant women with thyroid dysfunction, supports its clinical application in specific populations, such as SCH patients with positive TPOAb or TSH > 4.0 mU/l, and warns against the risk of overtreatment. The results of this study provide an evidence base for clinical precision intervention. Future studies should address the heterogeneity through standardized large studies, clarify the dose threshold, and evaluate the long-term health effects of LT4 on mothers and infants, to further improve the guidelines and optimize risk stratification management.</p><p><strong>Study funding/competing interests: </strong>This work was supported by the National Key R&D Program of China (Grant No. 2023YFC2508300, 2023YFC2508303, and 2023YFC2508305), the National Science and Technology Major Project (Grant No. 2024ZD0533403), and the National Natural Science Foundation of China (Grant No. 82100831, 81570709, and 82470826). All authors declared no competing interests.</p><p><strong>Registration number: </strong>CRD42024586105.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2025 3","pages":"hoaf036"},"PeriodicalIF":11.1000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12448225/pdf/","citationCount":"0","resultStr":"{\"title\":\"Levothyroxine supplementation and pregnancy outcomes in women with thyroid disorders: an umbrella review of systematic reviews and meta-analyses of randomized controlled trials.\",\"authors\":\"Jing Wang, Jiashu Li, Jing Zhang, Aihua Liu, Wanyu Yang, Xiaodan Zhai, Weiping Teng, Yongze Li, Zhongyan Shan\",\"doi\":\"10.1093/hropen/hoaf036\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study question: </strong>Does levothyroxine (LT4) treatment reduce adverse pregnancy outcomes in pregnant women with thyroid dysfunction?</p><p><strong>Summary answer: </strong>LT4 treatment significantly reduces the risks of pregnancy loss, preterm delivery, and gestational hypertension, with no significant impacts on rates of live birth, placental abruption, or gestational diabetes.</p><p><strong>What is known already: </strong>Multiple meta-analyses have examined the impact of LT4 on pregnancy outcomes, but quantitative confidence assessments are still lacking. Thus, an umbrella review is needed to systematically synthesize and assess the quality of this evidence.</p><p><strong>Study design size duration: </strong>This umbrella review of systematic reviews and meta-analyses used PubMed, Embase, Web of Science, and the Cochrane Database of Systematic Reviews. Searches included studies published in English or Chinese up to 20 March 2025.</p><p><strong>Participants/materials setting methods: </strong>Included studies were systematic reviews or meta-analyses of randomized controlled trials assessing the effects of LT4 on pregnancy outcomes in women with subclinical hypothyroidism (SCH) or thyroid peroxidase antibody (TPOAb) positivity. A set of 24 associations across six pregnancy outcomes were analyzed: pregnancy loss, preterm delivery, live birth, placental abruption, gestational hypertension, and gestational diabetes. Methodological quality was assessed using AMSTAR 1, and evidence quality was graded using GRADE. Sensitivity analyses were conducted to confirm robustness.</p><p><strong>Main results and the role of chance: </strong>Eleven meta-analyses were included. High-quality evidence showed that LT4 treatment reduced the risks of pregnancy loss (RR = 0.43; class III evidence), preterm delivery (RR = 0.56; class III evidence), and gestational hypertension (RR = 0.63; class IV evidence). Moderate-to-low-quality evidence indicated no significant impact on rates of live birth, placental abruption, or gestational diabetes. Of the 24 associations, 22 were rated as high confidence and two as medium confidence based on AMSTAR 1. Sensitivity analyses confirmed the robustness of the findings, but treatment effects varied according to the study population, treatment timing, and method. For pregnancy loss and preterm delivery outcomes, the risk was significantly reduced only when LT4 treatment was initiated in early pregnancy (pregnancy loss: RR = 0.60, <i>P</i> = 0.03; RR = 0.59, <i>P</i> = 0.003; preterm labor: RR = 0.58, <i>P </i>< 0.0001; RR = 0.46, <i>P</i> < 0.00001). Additionally, women with TSH levels greater than 4.0 mU/l derived greater benefits from LT4 treatment compared to those with TSH levels between 2.5 and 4.0 mU/l.</p><p><strong>Limitations reasons for caution: </strong>Limitations include small sample sizes, potential biases (selection and reporting), and language restrictions to English and Chinese studies, which may affect generalizability.</p><p><strong>Wider implications of the findings: </strong>By integrating high-quality evidence, this study confirms that LT4 can reduce the risk of pregnancy loss and preterm delivery in pregnant women with thyroid dysfunction, supports its clinical application in specific populations, such as SCH patients with positive TPOAb or TSH > 4.0 mU/l, and warns against the risk of overtreatment. The results of this study provide an evidence base for clinical precision intervention. Future studies should address the heterogeneity through standardized large studies, clarify the dose threshold, and evaluate the long-term health effects of LT4 on mothers and infants, to further improve the guidelines and optimize risk stratification management.</p><p><strong>Study funding/competing interests: </strong>This work was supported by the National Key R&D Program of China (Grant No. 2023YFC2508300, 2023YFC2508303, and 2023YFC2508305), the National Science and Technology Major Project (Grant No. 2024ZD0533403), and the National Natural Science Foundation of China (Grant No. 82100831, 81570709, and 82470826). All authors declared no competing interests.</p><p><strong>Registration number: </strong>CRD42024586105.</p>\",\"PeriodicalId\":73264,\"journal\":{\"name\":\"Human reproduction open\",\"volume\":\"2025 3\",\"pages\":\"hoaf036\"},\"PeriodicalIF\":11.1000,\"publicationDate\":\"2025-09-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12448225/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Human reproduction open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/hropen/hoaf036\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoaf036","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Levothyroxine supplementation and pregnancy outcomes in women with thyroid disorders: an umbrella review of systematic reviews and meta-analyses of randomized controlled trials.
Study question: Does levothyroxine (LT4) treatment reduce adverse pregnancy outcomes in pregnant women with thyroid dysfunction?
Summary answer: LT4 treatment significantly reduces the risks of pregnancy loss, preterm delivery, and gestational hypertension, with no significant impacts on rates of live birth, placental abruption, or gestational diabetes.
What is known already: Multiple meta-analyses have examined the impact of LT4 on pregnancy outcomes, but quantitative confidence assessments are still lacking. Thus, an umbrella review is needed to systematically synthesize and assess the quality of this evidence.
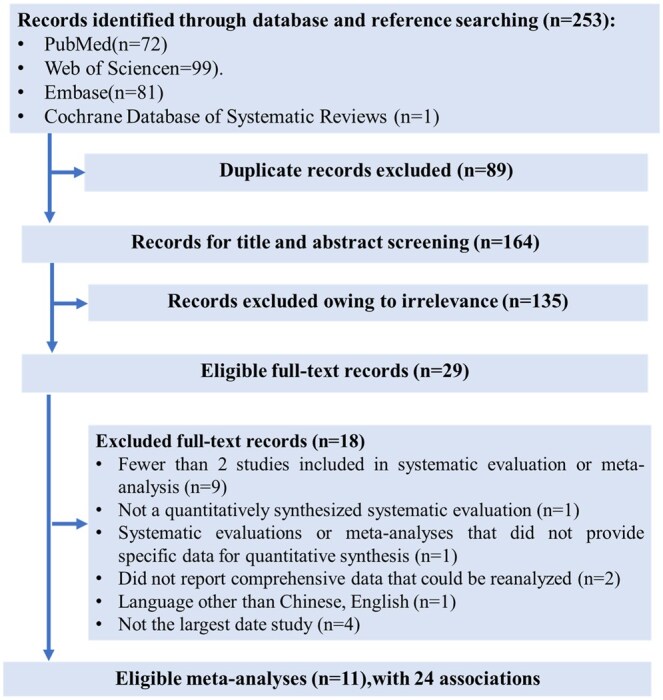
Study design size duration: This umbrella review of systematic reviews and meta-analyses used PubMed, Embase, Web of Science, and the Cochrane Database of Systematic Reviews. Searches included studies published in English or Chinese up to 20 March 2025.
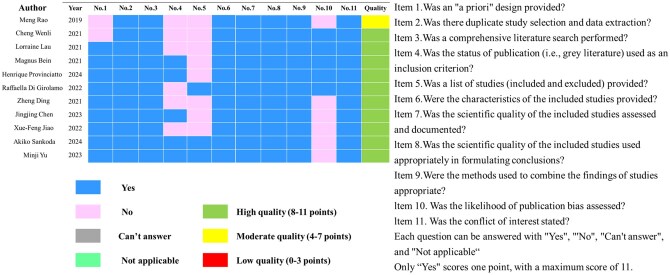
Participants/materials setting methods: Included studies were systematic reviews or meta-analyses of randomized controlled trials assessing the effects of LT4 on pregnancy outcomes in women with subclinical hypothyroidism (SCH) or thyroid peroxidase antibody (TPOAb) positivity. A set of 24 associations across six pregnancy outcomes were analyzed: pregnancy loss, preterm delivery, live birth, placental abruption, gestational hypertension, and gestational diabetes. Methodological quality was assessed using AMSTAR 1, and evidence quality was graded using GRADE. Sensitivity analyses were conducted to confirm robustness.
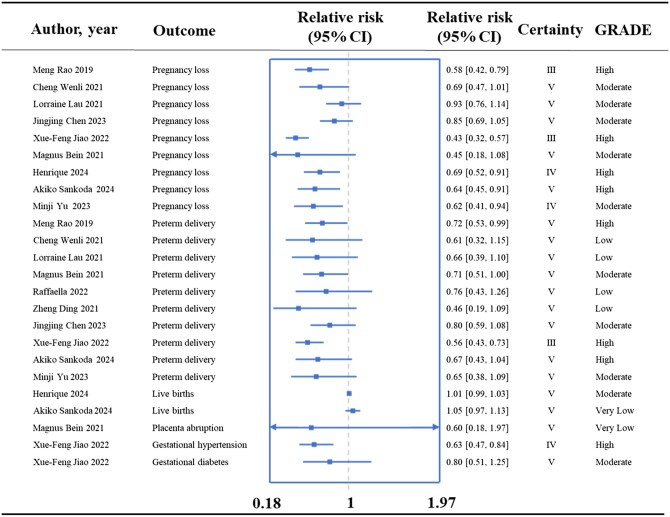
Main results and the role of chance: Eleven meta-analyses were included. High-quality evidence showed that LT4 treatment reduced the risks of pregnancy loss (RR = 0.43; class III evidence), preterm delivery (RR = 0.56; class III evidence), and gestational hypertension (RR = 0.63; class IV evidence). Moderate-to-low-quality evidence indicated no significant impact on rates of live birth, placental abruption, or gestational diabetes. Of the 24 associations, 22 were rated as high confidence and two as medium confidence based on AMSTAR 1. Sensitivity analyses confirmed the robustness of the findings, but treatment effects varied according to the study population, treatment timing, and method. For pregnancy loss and preterm delivery outcomes, the risk was significantly reduced only when LT4 treatment was initiated in early pregnancy (pregnancy loss: RR = 0.60, P = 0.03; RR = 0.59, P = 0.003; preterm labor: RR = 0.58, P < 0.0001; RR = 0.46, P < 0.00001). Additionally, women with TSH levels greater than 4.0 mU/l derived greater benefits from LT4 treatment compared to those with TSH levels between 2.5 and 4.0 mU/l.
Limitations reasons for caution: Limitations include small sample sizes, potential biases (selection and reporting), and language restrictions to English and Chinese studies, which may affect generalizability.
Wider implications of the findings: By integrating high-quality evidence, this study confirms that LT4 can reduce the risk of pregnancy loss and preterm delivery in pregnant women with thyroid dysfunction, supports its clinical application in specific populations, such as SCH patients with positive TPOAb or TSH > 4.0 mU/l, and warns against the risk of overtreatment. The results of this study provide an evidence base for clinical precision intervention. Future studies should address the heterogeneity through standardized large studies, clarify the dose threshold, and evaluate the long-term health effects of LT4 on mothers and infants, to further improve the guidelines and optimize risk stratification management.
Study funding/competing interests: This work was supported by the National Key R&D Program of China (Grant No. 2023YFC2508300, 2023YFC2508303, and 2023YFC2508305), the National Science and Technology Major Project (Grant No. 2024ZD0533403), and the National Natural Science Foundation of China (Grant No. 82100831, 81570709, and 82470826). All authors declared no competing interests.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


