Rishi Pawa, Nicholas Koutlas, Alexa Cecil, Robert Dorrell, Gregory Russell, Swati Pawa
{"title":"急性胆囊炎高危患者eus引导胆囊引流与经皮胆囊引流:倾向评分匹配分析","authors":"Rishi Pawa, Nicholas Koutlas, Alexa Cecil, Robert Dorrell, Gregory Russell, Swati Pawa","doi":"10.1177/17562848251375376","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) using lumen apposing metal stent (LAMS) has emerged as a treatment option in patients with acute cholecystitis (AC) deemed unfit for surgery. Prior to this technique, percutaneous transhepatic gallbladder drainage (PT-GBD) was the only drainage modality available for these patients.</p><p><strong>Objectives: </strong>This study compares clinical outcomes of EUS-GBD versus PT-GBD in high-risk surgical patients with AC.</p><p><strong>Design: </strong>From July 2019 to October 2023, all consecutive patients with AC undergoing EUS-GBD (using LAMS) and PT-GBD at a single academic medical center were retrospectively reviewed and analyzed.</p><p><strong>Methods: </strong>A propensity score-matched analysis using age, sex, and Charlson Comorbidity Index was performed. This was used to obtain a 1:1 ratio of PT-GBD:EUS-GBD patients. Technical success was defined as successful placement of LAMS or percutaneous cholecystostomy tube in the gallbladder. Clinical success was defined as resolution of patients' symptoms and normalization of white cell count within 96 h post procedure without recurrence of AC. Outcomes were analyzed using Fisher's exact test and Student's <i>t</i> test.</p><p><strong>Results: </strong>Following propensity score matching, 57 EUS-GBD patients were matched with 57 PT-GBD patients. Technical success was seen in 96% (55/57) in the EUS-GBD group and 98% (56/57) in the PT-GBD group (<i>p</i> > 0.99). Clinical success was observed in 93% (52/56) in EUS-GBD group and 80% (45/56) in PT-GBD group (<i>p</i> = 0.093). PT-GBD patients underwent more procedures than the EUS-GBD group (median 3 vs 2, <i>p</i> < 0.0001) and had more complications (44% vs 16%, <i>p</i> = 0.0010). The median survival was 573 days for EUS-GBD and 452 days for PT-GBD (<i>p</i> = 0.77).</p><p><strong>Conclusion: </strong>EUS-GBD is superior to PT-GBD, requiring fewer gallbladder-related procedures and lower rates of adverse events. Given these benefits, it has emerged as the preferred non-surgical alternative in the management of patients with AC who are poor surgical candidates.</p>","PeriodicalId":48770,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"18 ","pages":"17562848251375376"},"PeriodicalIF":3.4000,"publicationDate":"2025-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12449632/pdf/","citationCount":"0","resultStr":"{\"title\":\"EUS-guided gallbladder drainage versus percutaneous gallbladder drainage in high-risk patients with acute cholecystitis: a propensity score-matched analysis.\",\"authors\":\"Rishi Pawa, Nicholas Koutlas, Alexa Cecil, Robert Dorrell, Gregory Russell, Swati Pawa\",\"doi\":\"10.1177/17562848251375376\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) using lumen apposing metal stent (LAMS) has emerged as a treatment option in patients with acute cholecystitis (AC) deemed unfit for surgery. Prior to this technique, percutaneous transhepatic gallbladder drainage (PT-GBD) was the only drainage modality available for these patients.</p><p><strong>Objectives: </strong>This study compares clinical outcomes of EUS-GBD versus PT-GBD in high-risk surgical patients with AC.</p><p><strong>Design: </strong>From July 2019 to October 2023, all consecutive patients with AC undergoing EUS-GBD (using LAMS) and PT-GBD at a single academic medical center were retrospectively reviewed and analyzed.</p><p><strong>Methods: </strong>A propensity score-matched analysis using age, sex, and Charlson Comorbidity Index was performed. This was used to obtain a 1:1 ratio of PT-GBD:EUS-GBD patients. Technical success was defined as successful placement of LAMS or percutaneous cholecystostomy tube in the gallbladder. Clinical success was defined as resolution of patients' symptoms and normalization of white cell count within 96 h post procedure without recurrence of AC. Outcomes were analyzed using Fisher's exact test and Student's <i>t</i> test.</p><p><strong>Results: </strong>Following propensity score matching, 57 EUS-GBD patients were matched with 57 PT-GBD patients. Technical success was seen in 96% (55/57) in the EUS-GBD group and 98% (56/57) in the PT-GBD group (<i>p</i> > 0.99). Clinical success was observed in 93% (52/56) in EUS-GBD group and 80% (45/56) in PT-GBD group (<i>p</i> = 0.093). PT-GBD patients underwent more procedures than the EUS-GBD group (median 3 vs 2, <i>p</i> < 0.0001) and had more complications (44% vs 16%, <i>p</i> = 0.0010). The median survival was 573 days for EUS-GBD and 452 days for PT-GBD (<i>p</i> = 0.77).</p><p><strong>Conclusion: </strong>EUS-GBD is superior to PT-GBD, requiring fewer gallbladder-related procedures and lower rates of adverse events. Given these benefits, it has emerged as the preferred non-surgical alternative in the management of patients with AC who are poor surgical candidates.</p>\",\"PeriodicalId\":48770,\"journal\":{\"name\":\"Therapeutic Advances in Gastroenterology\",\"volume\":\"18 \",\"pages\":\"17562848251375376\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12449632/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562848251375376\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848251375376","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:超声内镜下胆囊引流(EUS-GBD)使用腔旁金属支架(LAMS)已成为急性胆囊炎(AC)患者认为不适合手术的治疗选择。在此技术之前,经皮经肝胆囊引流(PT-GBD)是这些患者唯一可用的引流方式。设计:从2019年7月至2023年10月,回顾性分析在单一学术医疗中心连续接受EUS-GBD(使用LAMS)和PT-GBD的所有AC患者。方法:使用年龄、性别和Charlson合并症指数进行倾向评分匹配分析。该方法用于获得PT-GBD:EUS-GBD患者的1:1比例。技术上的成功定义为在胆囊内成功放置LAMS或经皮胆囊造瘘管。临床成功定义为患者症状的缓解和术后96小时内白细胞计数的正常化,无AC复发。使用Fisher精确检验和学生t检验分析结果。结果:根据倾向评分匹配,57例EUS-GBD患者与57例PT-GBD患者匹配。EUS-GBD组技术成功率为96% (55/57),PT-GBD组技术成功率为98% (56/57)(p < 0.99)。EUS-GBD组临床成功率为93% (52/56),PT-GBD组临床成功率为80% (45/56)(p = 0.093)。PT-GBD患者比EUS-GBD组接受了更多的手术(中位数3 vs 2, p p = 0.0010)。EUS-GBD的中位生存期为573天,PT-GBD的中位生存期为452天(p = 0.77)。结论:EUS-GBD优于PT-GBD,需要较少的胆囊相关手术和较低的不良事件发生率。鉴于这些好处,它已成为治疗不适合手术治疗的AC患者首选的非手术治疗方法。
EUS-guided gallbladder drainage versus percutaneous gallbladder drainage in high-risk patients with acute cholecystitis: a propensity score-matched analysis.
Background: Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) using lumen apposing metal stent (LAMS) has emerged as a treatment option in patients with acute cholecystitis (AC) deemed unfit for surgery. Prior to this technique, percutaneous transhepatic gallbladder drainage (PT-GBD) was the only drainage modality available for these patients.
Objectives: This study compares clinical outcomes of EUS-GBD versus PT-GBD in high-risk surgical patients with AC.
Design: From July 2019 to October 2023, all consecutive patients with AC undergoing EUS-GBD (using LAMS) and PT-GBD at a single academic medical center were retrospectively reviewed and analyzed.
Methods: A propensity score-matched analysis using age, sex, and Charlson Comorbidity Index was performed. This was used to obtain a 1:1 ratio of PT-GBD:EUS-GBD patients. Technical success was defined as successful placement of LAMS or percutaneous cholecystostomy tube in the gallbladder. Clinical success was defined as resolution of patients' symptoms and normalization of white cell count within 96 h post procedure without recurrence of AC. Outcomes were analyzed using Fisher's exact test and Student's t test.
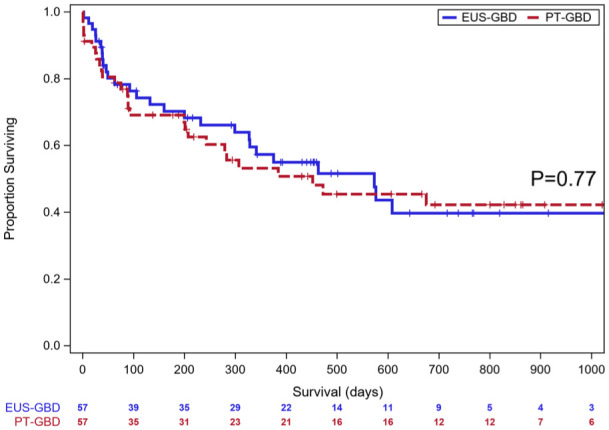
Results: Following propensity score matching, 57 EUS-GBD patients were matched with 57 PT-GBD patients. Technical success was seen in 96% (55/57) in the EUS-GBD group and 98% (56/57) in the PT-GBD group (p > 0.99). Clinical success was observed in 93% (52/56) in EUS-GBD group and 80% (45/56) in PT-GBD group (p = 0.093). PT-GBD patients underwent more procedures than the EUS-GBD group (median 3 vs 2, p < 0.0001) and had more complications (44% vs 16%, p = 0.0010). The median survival was 573 days for EUS-GBD and 452 days for PT-GBD (p = 0.77).
Conclusion: EUS-GBD is superior to PT-GBD, requiring fewer gallbladder-related procedures and lower rates of adverse events. Given these benefits, it has emerged as the preferred non-surgical alternative in the management of patients with AC who are poor surgical candidates.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


