Tesfaye H Leta, Richard N Chang, Stein Atle Lie, Anne Marie Fenstad, Stein Håkon L Lygre, Martin Lindberg-Larsen, Alma B Pedersen, Annette W-Dahl, Ola Rolfson, Oskar Johansson, Liza N van Steenbergen, Rob Ghh Nelissen, Dylan Harries, Carl Holder, Peter Lewis, Richard de Steiger, Olav Lutro, Keijo Mäkelä, Mikko S Venäläinen, Jinny Willis, Chris Frampton, Michael Wyatt, Alexander Grimberg, Arnd Steinbrück, Yinan Wu, Håvard Dale, Christian Brand, Bernhard Christen, Joanne Shapiro, J Mark Wilkinson, Morgan Edwards, Geir Hallan, Jan-Erik Gjertsen, Ove Furnes, Art Sedrakyan, Heather A Prentice, Elizabeth W Paxton
{"title":"高风险患者膝关节置换术后抗生素骨水泥与感染风险:基于登记的荟萃分析。","authors":"Tesfaye H Leta, Richard N Chang, Stein Atle Lie, Anne Marie Fenstad, Stein Håkon L Lygre, Martin Lindberg-Larsen, Alma B Pedersen, Annette W-Dahl, Ola Rolfson, Oskar Johansson, Liza N van Steenbergen, Rob Ghh Nelissen, Dylan Harries, Carl Holder, Peter Lewis, Richard de Steiger, Olav Lutro, Keijo Mäkelä, Mikko S Venäläinen, Jinny Willis, Chris Frampton, Michael Wyatt, Alexander Grimberg, Arnd Steinbrück, Yinan Wu, Håvard Dale, Christian Brand, Bernhard Christen, Joanne Shapiro, J Mark Wilkinson, Morgan Edwards, Geir Hallan, Jan-Erik Gjertsen, Ove Furnes, Art Sedrakyan, Heather A Prentice, Elizabeth W Paxton","doi":"10.2106/JBJS.OA.25.00061","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of antibiotic-loaded bone cement (ALBC) in primary total knee arthroplasty (TKA) is debated. Some argue that ALBC might only be justified in high-risk patients. This study assessed the effectiveness of ALBC vs. plain bone cement (PBC) in reducing risk of revision for periprosthetic joint infection (PJI) in TKA patients considered to have a high risk of infection.</p><p><strong>Methods: </strong>Cohort study of primary TKAs in 11 national or regional arthroplasty registries from 2010 to 2020. The 1-year risk of revision for PJI in TKAs with ALBC vs. PBC among patients with high American Society of Anesthesiologists (ASA) classification, body mass index (BMI), and/or diabetes was compared. Cumulative percent revision (1 minus Kaplan-Meier) based on 685,818 TKAs and Cox regression analyses (adjusted Hazard Rate Ratios [aHRRs]) were performed for TKAs with ALBC (reference) vs. PBC restricted to the following high-risk subgroups of patients: (1) ASA ≥3 (n = 335,612 vs. 35,997), (2) BMI ≥35 (n = 278,927 vs. 24,737), (3) ASA ≥3 and BMI ≥35 (n = 99,407 vs. 11,407), (4) diabetes (n = 38,341 vs. 21,838), and (5) ASA ≥3, BMI ≥35, and diabetes (n = 3,347 vs. 4,261). Advanced distributed meta-analyses were performed to combine all aggregate data and assess 1-year risk of revision for PJI.</p><p><strong>Results: </strong>Each registry reported a 1-year cumulative percent revision of ≤1.6% for PJI following TKAs both for ALBC and PBC in all high-risk subgroups. Similar 1-year risks of revision for PJI were found in TKAs with ALBC (reference) and PBC among patients with ASA ≥3 (aHRR: 1.09; 95% CI, 0.90-1.31); BMI ≥35 (1.06; 0.54-2.12); ASA ≥3 and BMI ≥35 (1.12; 0.83-1.50); diabetes (0.95; 0.74-1.20); and ASA ≥3, BMI ≥35, and diabetes (1.40; 0.86-2.29).</p><p><strong>Conclusions and relevance: </strong>Similar 1-year revision risk of PJI was found for TKAs with ALBC vs. PBC in high-risk patients. Confirmation of the efficacy of ALBC in high-risk TKA patients needs to be evaluated in clinical trials.</p><p><strong>Level of evidence: </strong>Level III. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 3","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12443158/pdf/","citationCount":"0","resultStr":"{\"title\":\"Antibiotic-Loaded Bone Cement and Risk of Infection After Knee Arthroplasty in High-Risk Patients: A Register Based Meta-Analysis.\",\"authors\":\"Tesfaye H Leta, Richard N Chang, Stein Atle Lie, Anne Marie Fenstad, Stein Håkon L Lygre, Martin Lindberg-Larsen, Alma B Pedersen, Annette W-Dahl, Ola Rolfson, Oskar Johansson, Liza N van Steenbergen, Rob Ghh Nelissen, Dylan Harries, Carl Holder, Peter Lewis, Richard de Steiger, Olav Lutro, Keijo Mäkelä, Mikko S Venäläinen, Jinny Willis, Chris Frampton, Michael Wyatt, Alexander Grimberg, Arnd Steinbrück, Yinan Wu, Håvard Dale, Christian Brand, Bernhard Christen, Joanne Shapiro, J Mark Wilkinson, Morgan Edwards, Geir Hallan, Jan-Erik Gjertsen, Ove Furnes, Art Sedrakyan, Heather A Prentice, Elizabeth W Paxton\",\"doi\":\"10.2106/JBJS.OA.25.00061\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The use of antibiotic-loaded bone cement (ALBC) in primary total knee arthroplasty (TKA) is debated. Some argue that ALBC might only be justified in high-risk patients. This study assessed the effectiveness of ALBC vs. plain bone cement (PBC) in reducing risk of revision for periprosthetic joint infection (PJI) in TKA patients considered to have a high risk of infection.</p><p><strong>Methods: </strong>Cohort study of primary TKAs in 11 national or regional arthroplasty registries from 2010 to 2020. The 1-year risk of revision for PJI in TKAs with ALBC vs. PBC among patients with high American Society of Anesthesiologists (ASA) classification, body mass index (BMI), and/or diabetes was compared. Cumulative percent revision (1 minus Kaplan-Meier) based on 685,818 TKAs and Cox regression analyses (adjusted Hazard Rate Ratios [aHRRs]) were performed for TKAs with ALBC (reference) vs. PBC restricted to the following high-risk subgroups of patients: (1) ASA ≥3 (n = 335,612 vs. 35,997), (2) BMI ≥35 (n = 278,927 vs. 24,737), (3) ASA ≥3 and BMI ≥35 (n = 99,407 vs. 11,407), (4) diabetes (n = 38,341 vs. 21,838), and (5) ASA ≥3, BMI ≥35, and diabetes (n = 3,347 vs. 4,261). Advanced distributed meta-analyses were performed to combine all aggregate data and assess 1-year risk of revision for PJI.</p><p><strong>Results: </strong>Each registry reported a 1-year cumulative percent revision of ≤1.6% for PJI following TKAs both for ALBC and PBC in all high-risk subgroups. Similar 1-year risks of revision for PJI were found in TKAs with ALBC (reference) and PBC among patients with ASA ≥3 (aHRR: 1.09; 95% CI, 0.90-1.31); BMI ≥35 (1.06; 0.54-2.12); ASA ≥3 and BMI ≥35 (1.12; 0.83-1.50); diabetes (0.95; 0.74-1.20); and ASA ≥3, BMI ≥35, and diabetes (1.40; 0.86-2.29).</p><p><strong>Conclusions and relevance: </strong>Similar 1-year revision risk of PJI was found for TKAs with ALBC vs. PBC in high-risk patients. Confirmation of the efficacy of ALBC in high-risk TKA patients needs to be evaluated in clinical trials.</p><p><strong>Level of evidence: </strong>Level III. See Instructions for Authors for a complete description of levels of evidence.</p>\",\"PeriodicalId\":36492,\"journal\":{\"name\":\"JBJS Open Access\",\"volume\":\"10 3\",\"pages\":\"\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-09-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12443158/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBJS Open Access\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2106/JBJS.OA.25.00061\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.25.00061","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Antibiotic-Loaded Bone Cement and Risk of Infection After Knee Arthroplasty in High-Risk Patients: A Register Based Meta-Analysis.
Background: The use of antibiotic-loaded bone cement (ALBC) in primary total knee arthroplasty (TKA) is debated. Some argue that ALBC might only be justified in high-risk patients. This study assessed the effectiveness of ALBC vs. plain bone cement (PBC) in reducing risk of revision for periprosthetic joint infection (PJI) in TKA patients considered to have a high risk of infection.
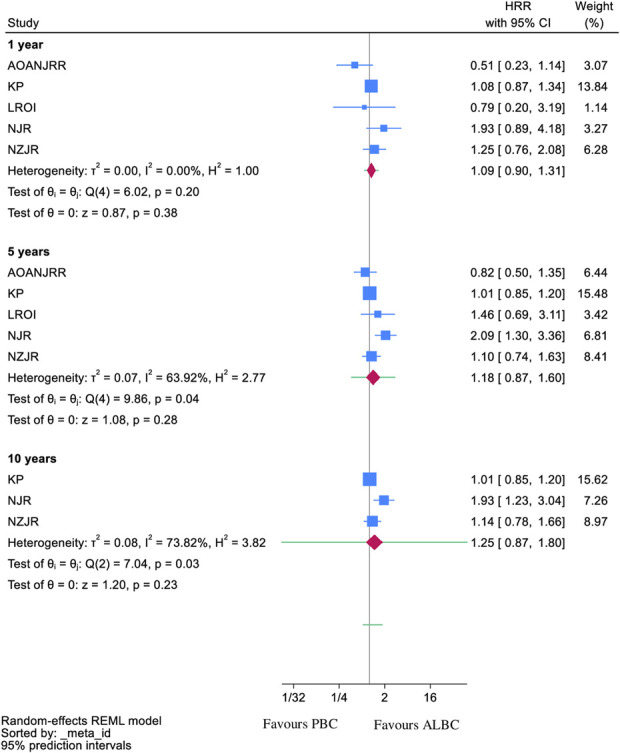
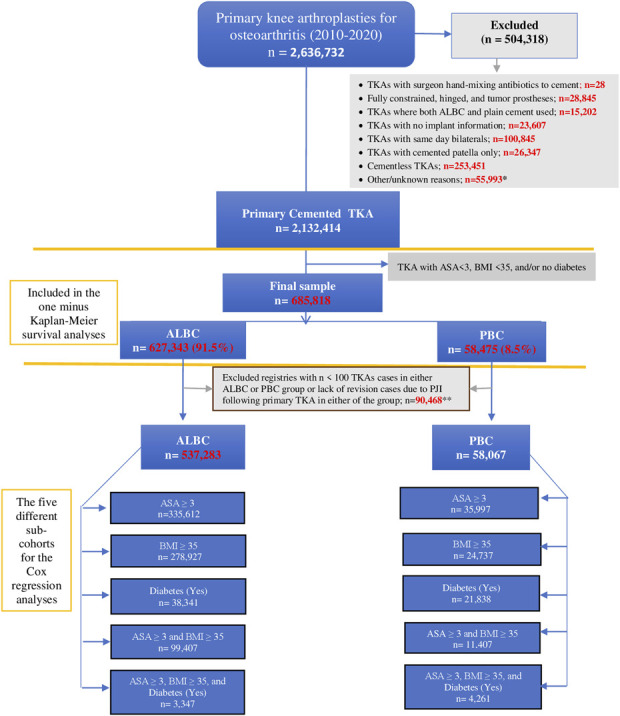
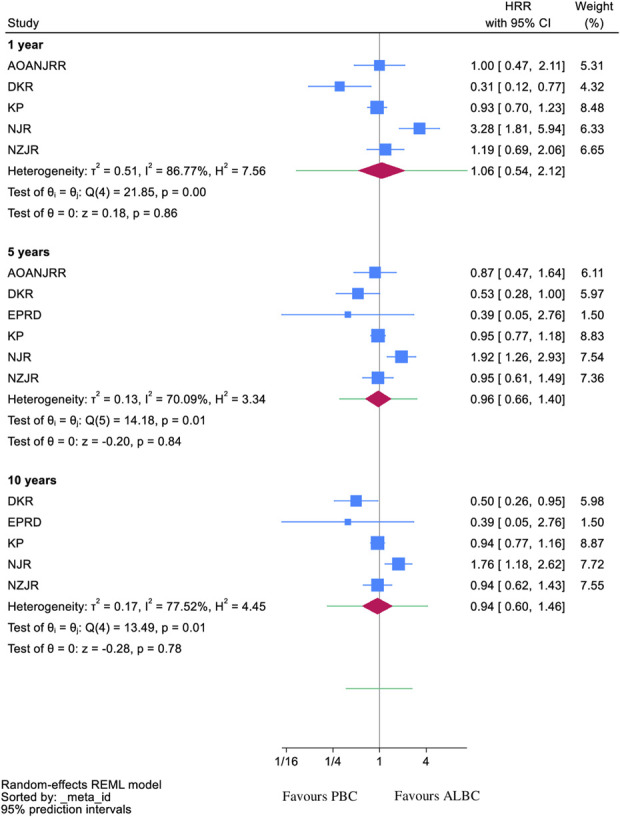
Methods: Cohort study of primary TKAs in 11 national or regional arthroplasty registries from 2010 to 2020. The 1-year risk of revision for PJI in TKAs with ALBC vs. PBC among patients with high American Society of Anesthesiologists (ASA) classification, body mass index (BMI), and/or diabetes was compared. Cumulative percent revision (1 minus Kaplan-Meier) based on 685,818 TKAs and Cox regression analyses (adjusted Hazard Rate Ratios [aHRRs]) were performed for TKAs with ALBC (reference) vs. PBC restricted to the following high-risk subgroups of patients: (1) ASA ≥3 (n = 335,612 vs. 35,997), (2) BMI ≥35 (n = 278,927 vs. 24,737), (3) ASA ≥3 and BMI ≥35 (n = 99,407 vs. 11,407), (4) diabetes (n = 38,341 vs. 21,838), and (5) ASA ≥3, BMI ≥35, and diabetes (n = 3,347 vs. 4,261). Advanced distributed meta-analyses were performed to combine all aggregate data and assess 1-year risk of revision for PJI.
Results: Each registry reported a 1-year cumulative percent revision of ≤1.6% for PJI following TKAs both for ALBC and PBC in all high-risk subgroups. Similar 1-year risks of revision for PJI were found in TKAs with ALBC (reference) and PBC among patients with ASA ≥3 (aHRR: 1.09; 95% CI, 0.90-1.31); BMI ≥35 (1.06; 0.54-2.12); ASA ≥3 and BMI ≥35 (1.12; 0.83-1.50); diabetes (0.95; 0.74-1.20); and ASA ≥3, BMI ≥35, and diabetes (1.40; 0.86-2.29).
Conclusions and relevance: Similar 1-year revision risk of PJI was found for TKAs with ALBC vs. PBC in high-risk patients. Confirmation of the efficacy of ALBC in high-risk TKA patients needs to be evaluated in clinical trials.
Level of evidence: Level III. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


