Austin G Kulasekararaj, Jun-Ichi Nishimura, Alexander Röth, Leigh Beveridge, Simon Buatois, Muriel Buri, Nicolo Compagno, Yves Luder, Sasha Sreckovic, Phillip Scheinberg
{"title":"处理阵发性夜间血红蛋白尿患者的短暂免疫复合物反应:来自COMMODORE 1和2研究的临床观察","authors":"Austin G Kulasekararaj, Jun-Ichi Nishimura, Alexander Röth, Leigh Beveridge, Simon Buatois, Muriel Buri, Nicolo Compagno, Yves Luder, Sasha Sreckovic, Phillip Scheinberg","doi":"10.1177/20406207251359246","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Crovalimab is a novel C5 inhibitor that enables rapid and sustained C5 inhibition with every 4-week subcutaneous maintenance dosing, with the possibility for self-administration. When switching from another C5 inhibitor (binds to a different epitope than crovalimab) to crovalimab and vice versa, transient immune complexes will form and may cause transient immune complex reactions (TICRs).</p><p><strong>Objectives: </strong>To assess TICR occurrence, manifestation, and management in patients with paroxysmal nocturnal hemoglobinuria (PNH) who switched from another C5 inhibitor to crovalimab.</p><p><strong>Design: </strong>COMMODORE 1 and 2 randomized C5 inhibitor-experienced and -naïve patients, respectively, to receive crovalimab or eculizumab. The COMMODORE 1 nonrandomized, descriptive cohort included patients who previously received ravulizumab or approved or higher-than-approved doses of eculizumab.</p><p><strong>Methods: </strong>Pooled data of patients who switched from eculizumab or ravulizumab to crovalimab were evaluated for TICR incidence and severity. TICR treatments and TICR durations were assessed by severity.</p><p><strong>Results: </strong>This descriptive analysis included 201 patients who switched from eculizumab (<i>n</i> = 174) or ravulizumab (<i>n</i> = 27) to crovalimab. Baseline characteristics were generally balanced between patients with and without a TICR. Thirty-nine of 201 patients (19%) experienced TICRs (11% Grades 1-2; 8% Grade 3; no Grades 4-5). Median time to onset and median TICR duration were 1.6 (range, 0.7-4.4) and 1.7 weeks (range, 0.4-34.1), respectively. The most common symptoms were arthralgia (45%), rash (34%), and pyrexia (21%), with no evidence of renal manifestations. Oral corticosteroids were the most common TICR treatment. Grade 3 TICRs were treated with higher oral corticosteroid dose but did not take longer to resolve than Grades 1-2 TICRs.</p><p><strong>Conclusion: </strong>Pooled COMMODORE 1 and 2 data show that TICRs from switching between C5 inhibitors were generally mild to moderate and resolved with appropriate treatment. These results further confirm that crovalimab is well tolerated in patients with PNH.</p><p><strong>Trial registration: </strong>NCT04432584; NCT04434092.</p>","PeriodicalId":23048,"journal":{"name":"Therapeutic Advances in Hematology","volume":"16 ","pages":"20406207251359246"},"PeriodicalIF":3.1000,"publicationDate":"2025-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12444074/pdf/","citationCount":"0","resultStr":"{\"title\":\"Managing transient immune complex reactions in patients with paroxysmal nocturnal hemoglobinuria: clinical observations from the COMMODORE 1 and 2 studies.\",\"authors\":\"Austin G Kulasekararaj, Jun-Ichi Nishimura, Alexander Röth, Leigh Beveridge, Simon Buatois, Muriel Buri, Nicolo Compagno, Yves Luder, Sasha Sreckovic, Phillip Scheinberg\",\"doi\":\"10.1177/20406207251359246\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Crovalimab is a novel C5 inhibitor that enables rapid and sustained C5 inhibition with every 4-week subcutaneous maintenance dosing, with the possibility for self-administration. When switching from another C5 inhibitor (binds to a different epitope than crovalimab) to crovalimab and vice versa, transient immune complexes will form and may cause transient immune complex reactions (TICRs).</p><p><strong>Objectives: </strong>To assess TICR occurrence, manifestation, and management in patients with paroxysmal nocturnal hemoglobinuria (PNH) who switched from another C5 inhibitor to crovalimab.</p><p><strong>Design: </strong>COMMODORE 1 and 2 randomized C5 inhibitor-experienced and -naïve patients, respectively, to receive crovalimab or eculizumab. The COMMODORE 1 nonrandomized, descriptive cohort included patients who previously received ravulizumab or approved or higher-than-approved doses of eculizumab.</p><p><strong>Methods: </strong>Pooled data of patients who switched from eculizumab or ravulizumab to crovalimab were evaluated for TICR incidence and severity. TICR treatments and TICR durations were assessed by severity.</p><p><strong>Results: </strong>This descriptive analysis included 201 patients who switched from eculizumab (<i>n</i> = 174) or ravulizumab (<i>n</i> = 27) to crovalimab. Baseline characteristics were generally balanced between patients with and without a TICR. Thirty-nine of 201 patients (19%) experienced TICRs (11% Grades 1-2; 8% Grade 3; no Grades 4-5). Median time to onset and median TICR duration were 1.6 (range, 0.7-4.4) and 1.7 weeks (range, 0.4-34.1), respectively. The most common symptoms were arthralgia (45%), rash (34%), and pyrexia (21%), with no evidence of renal manifestations. Oral corticosteroids were the most common TICR treatment. Grade 3 TICRs were treated with higher oral corticosteroid dose but did not take longer to resolve than Grades 1-2 TICRs.</p><p><strong>Conclusion: </strong>Pooled COMMODORE 1 and 2 data show that TICRs from switching between C5 inhibitors were generally mild to moderate and resolved with appropriate treatment. These results further confirm that crovalimab is well tolerated in patients with PNH.</p><p><strong>Trial registration: </strong>NCT04432584; NCT04434092.</p>\",\"PeriodicalId\":23048,\"journal\":{\"name\":\"Therapeutic Advances in Hematology\",\"volume\":\"16 \",\"pages\":\"20406207251359246\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-09-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12444074/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/20406207251359246\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Hematology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20406207251359246","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Managing transient immune complex reactions in patients with paroxysmal nocturnal hemoglobinuria: clinical observations from the COMMODORE 1 and 2 studies.
Background: Crovalimab is a novel C5 inhibitor that enables rapid and sustained C5 inhibition with every 4-week subcutaneous maintenance dosing, with the possibility for self-administration. When switching from another C5 inhibitor (binds to a different epitope than crovalimab) to crovalimab and vice versa, transient immune complexes will form and may cause transient immune complex reactions (TICRs).
Objectives: To assess TICR occurrence, manifestation, and management in patients with paroxysmal nocturnal hemoglobinuria (PNH) who switched from another C5 inhibitor to crovalimab.
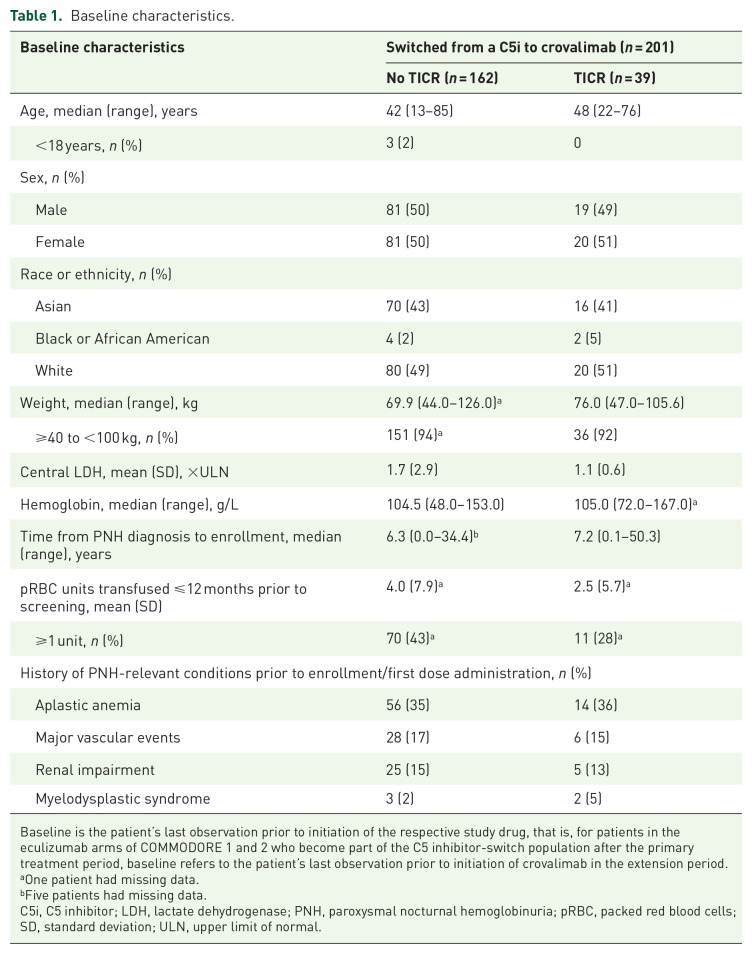
Design: COMMODORE 1 and 2 randomized C5 inhibitor-experienced and -naïve patients, respectively, to receive crovalimab or eculizumab. The COMMODORE 1 nonrandomized, descriptive cohort included patients who previously received ravulizumab or approved or higher-than-approved doses of eculizumab.
Methods: Pooled data of patients who switched from eculizumab or ravulizumab to crovalimab were evaluated for TICR incidence and severity. TICR treatments and TICR durations were assessed by severity.
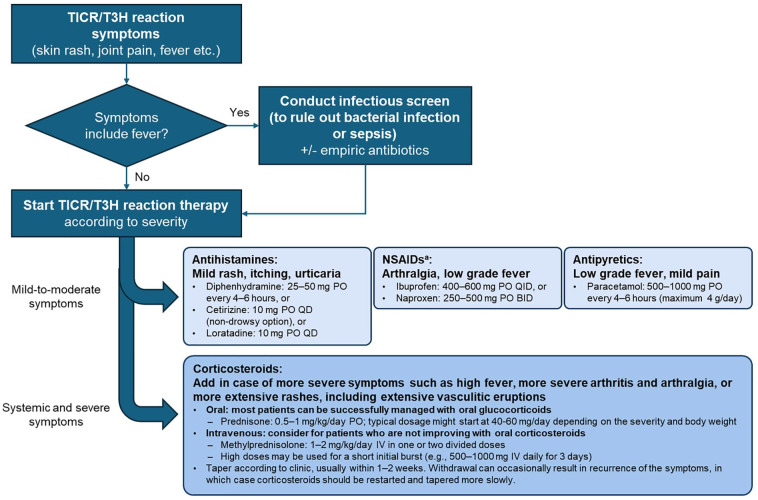
Results: This descriptive analysis included 201 patients who switched from eculizumab (n = 174) or ravulizumab (n = 27) to crovalimab. Baseline characteristics were generally balanced between patients with and without a TICR. Thirty-nine of 201 patients (19%) experienced TICRs (11% Grades 1-2; 8% Grade 3; no Grades 4-5). Median time to onset and median TICR duration were 1.6 (range, 0.7-4.4) and 1.7 weeks (range, 0.4-34.1), respectively. The most common symptoms were arthralgia (45%), rash (34%), and pyrexia (21%), with no evidence of renal manifestations. Oral corticosteroids were the most common TICR treatment. Grade 3 TICRs were treated with higher oral corticosteroid dose but did not take longer to resolve than Grades 1-2 TICRs.
Conclusion: Pooled COMMODORE 1 and 2 data show that TICRs from switching between C5 inhibitors were generally mild to moderate and resolved with appropriate treatment. These results further confirm that crovalimab is well tolerated in patients with PNH.
期刊介绍:
Therapeutic Advances in Hematology delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of hematology. The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in hematology, providing a forum in print and online for publishing the highest quality articles in this area.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


