{"title":"长骨角旋合并畸形单切口斜截骨准确垂直定位的几何规则是什么?","authors":"Balachandar Gopalan","doi":"10.5005/jp-journals-10080-1638","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Single-cut inclined osteotomy for angulation-rotation (A-R) deformity in long bone has a known transverse orientation, which is opposite to the direction of rotational deformity. The geometric rule(s) to guide the vertical orientation is hitherto unknown.</p><p><strong>Materials and methods: </strong>Using cylinder-shaped non-hardening modelling clay, eight angular (coronal, sagittal and their combinations) and two rotational (internal and external) deformities yielding 16 A-R deformity pairs were simulated for a right-sided model. The magnitudes of A and R deformities were 45° each. Resultant magnitudes of vertical and transverse orientations of the single-cut were constant at 45° and 22.5°, respectively. Transverse rotational orientation of the cut was external for internal rotational deformity and, internal for external rotational deformity. Vertical orientation of the cut was ascending and descending for each of the 32 A-R deformity models. Outcome measure was visual contact between oblique cut surfaces.</p><p><strong>Results: </strong>After ascending cut and derotational correction, the A-R deformities that maintained contact were varus-internal rotation, procurvatum-internal rotation, varus-procurvatum-internal rotation, varus-recurvatum-internal rotation, valgus-external rotation, recurvatum-external rotation, valgus-recurvatum-external rotation and valgus-procurvatum-external rotation. After descending cut and derotational correction, the A-R deformities that maintained contact were valgus-internal rotation, recurvatum-internal rotation, valgus-recurvatum-internal rotation, valgus-procurvatum-internal rotation, varus-external rotation, procurvatum-external rotation, varus-procurvatum-external rotation and varus-recurvatum-external rotation.</p><p><strong>Conclusion: </strong>The geometric rules guiding the vertical orientation of single-cut inclined osteotomy in A-R deformity are:Complementary A-R deformity requires an ascending osteotomy.- Varus and/or procurvatum with internal rotation.- Valgus and/or recurvatum with external rotation.Compensatory A-R deformity requires a descending osteotomy.- Varus and/or procurvatum with external rotation.- Valgus and/or recurvatum with internal rotation.In an A-R deformity with dissociative angular components, coronal plane deformity supersedes sagittal plane deformity in dictating the vertical orientation of the osteotomy. This is irrespective of the magnitude of coronal deformity.- Varus-recurvatum with internal or external rotation.- Valgus-procurvatum with internal or external rotation.</p><p><strong>Clinical significance: </strong>The combination pattern of angular and rotational components (A-R) determines accurate vertical orientation of the cut.Application of the geometric rules bypasses (1) complex calculations, (2) multiple trial-and-error methods and (3) expensive bone models.These simple rules will enable surgeons to consider the appropriate inclined osteotomy for any A-R deformity in clinical practice.The utility of 3D-printed models would be appropriate to improve the precision of the cut before surgery.</p><p><strong>How to cite this article: </strong>Gopalan B. What is the Geometric Rule that Guides Accurate Vertical Orientation of the Single-cut Inclined Osteotomy in a Combined Angulation-rotation Deformity of Long Bone? Strategies Trauma Limb Reconstr 2025;20(1):11-16.</p>","PeriodicalId":21979,"journal":{"name":"Strategies in Trauma and Limb Reconstruction","volume":"20 1","pages":"11-16"},"PeriodicalIF":1.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445133/pdf/","citationCount":"0","resultStr":"{\"title\":\"What is the Geometric Rule that Guides Accurate Vertical Orientation of the Single-cut Inclined Osteotomy in a Combined Angulation-rotation Deformity of Long Bone?\",\"authors\":\"Balachandar Gopalan\",\"doi\":\"10.5005/jp-journals-10080-1638\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Single-cut inclined osteotomy for angulation-rotation (A-R) deformity in long bone has a known transverse orientation, which is opposite to the direction of rotational deformity. The geometric rule(s) to guide the vertical orientation is hitherto unknown.</p><p><strong>Materials and methods: </strong>Using cylinder-shaped non-hardening modelling clay, eight angular (coronal, sagittal and their combinations) and two rotational (internal and external) deformities yielding 16 A-R deformity pairs were simulated for a right-sided model. The magnitudes of A and R deformities were 45° each. Resultant magnitudes of vertical and transverse orientations of the single-cut were constant at 45° and 22.5°, respectively. Transverse rotational orientation of the cut was external for internal rotational deformity and, internal for external rotational deformity. Vertical orientation of the cut was ascending and descending for each of the 32 A-R deformity models. Outcome measure was visual contact between oblique cut surfaces.</p><p><strong>Results: </strong>After ascending cut and derotational correction, the A-R deformities that maintained contact were varus-internal rotation, procurvatum-internal rotation, varus-procurvatum-internal rotation, varus-recurvatum-internal rotation, valgus-external rotation, recurvatum-external rotation, valgus-recurvatum-external rotation and valgus-procurvatum-external rotation. After descending cut and derotational correction, the A-R deformities that maintained contact were valgus-internal rotation, recurvatum-internal rotation, valgus-recurvatum-internal rotation, valgus-procurvatum-internal rotation, varus-external rotation, procurvatum-external rotation, varus-procurvatum-external rotation and varus-recurvatum-external rotation.</p><p><strong>Conclusion: </strong>The geometric rules guiding the vertical orientation of single-cut inclined osteotomy in A-R deformity are:Complementary A-R deformity requires an ascending osteotomy.- Varus and/or procurvatum with internal rotation.- Valgus and/or recurvatum with external rotation.Compensatory A-R deformity requires a descending osteotomy.- Varus and/or procurvatum with external rotation.- Valgus and/or recurvatum with internal rotation.In an A-R deformity with dissociative angular components, coronal plane deformity supersedes sagittal plane deformity in dictating the vertical orientation of the osteotomy. This is irrespective of the magnitude of coronal deformity.- Varus-recurvatum with internal or external rotation.- Valgus-procurvatum with internal or external rotation.</p><p><strong>Clinical significance: </strong>The combination pattern of angular and rotational components (A-R) determines accurate vertical orientation of the cut.Application of the geometric rules bypasses (1) complex calculations, (2) multiple trial-and-error methods and (3) expensive bone models.These simple rules will enable surgeons to consider the appropriate inclined osteotomy for any A-R deformity in clinical practice.The utility of 3D-printed models would be appropriate to improve the precision of the cut before surgery.</p><p><strong>How to cite this article: </strong>Gopalan B. What is the Geometric Rule that Guides Accurate Vertical Orientation of the Single-cut Inclined Osteotomy in a Combined Angulation-rotation Deformity of Long Bone? Strategies Trauma Limb Reconstr 2025;20(1):11-16.</p>\",\"PeriodicalId\":21979,\"journal\":{\"name\":\"Strategies in Trauma and Limb Reconstruction\",\"volume\":\"20 1\",\"pages\":\"11-16\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445133/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Strategies in Trauma and Limb Reconstruction\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5005/jp-journals-10080-1638\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Strategies in Trauma and Limb Reconstruction","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5005/jp-journals-10080-1638","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
What is the Geometric Rule that Guides Accurate Vertical Orientation of the Single-cut Inclined Osteotomy in a Combined Angulation-rotation Deformity of Long Bone?
Background: Single-cut inclined osteotomy for angulation-rotation (A-R) deformity in long bone has a known transverse orientation, which is opposite to the direction of rotational deformity. The geometric rule(s) to guide the vertical orientation is hitherto unknown.
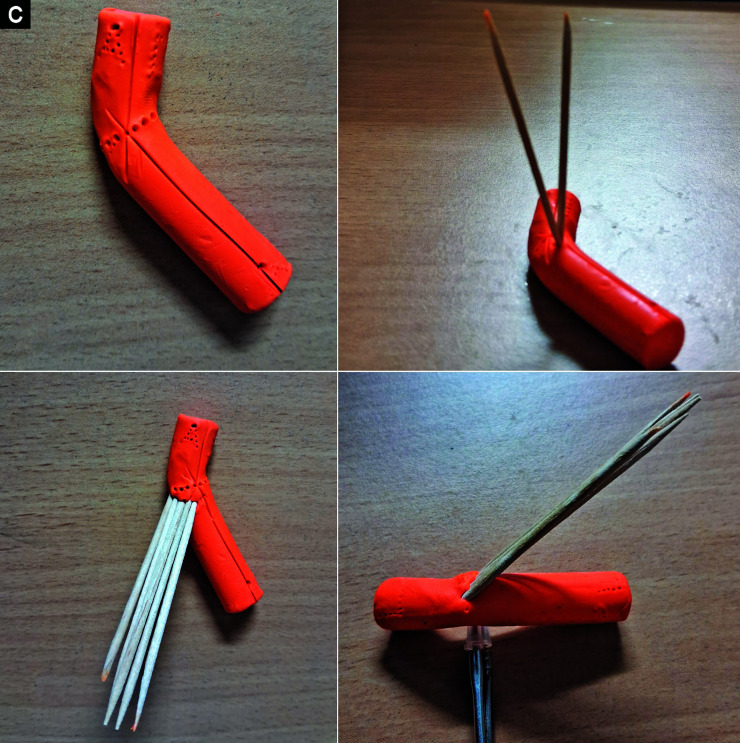
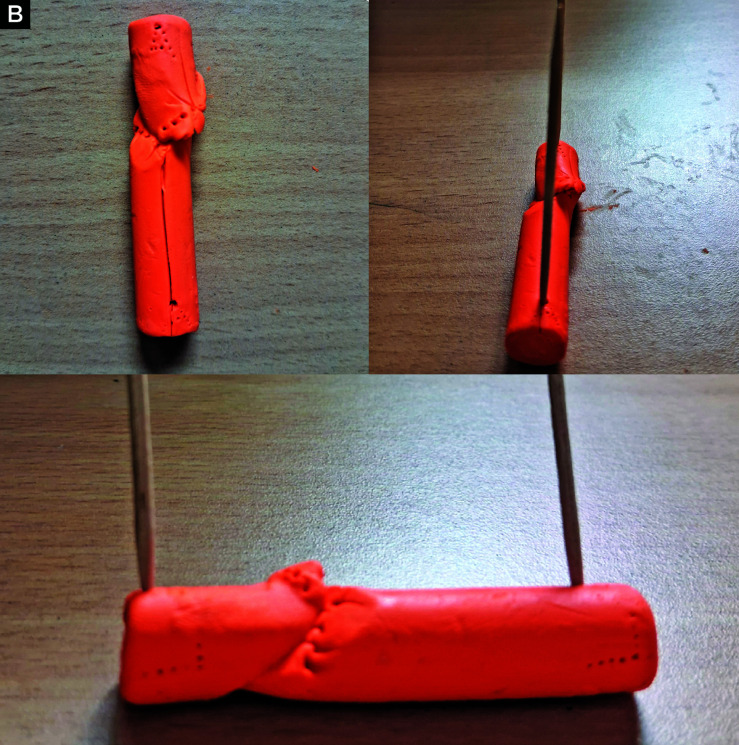
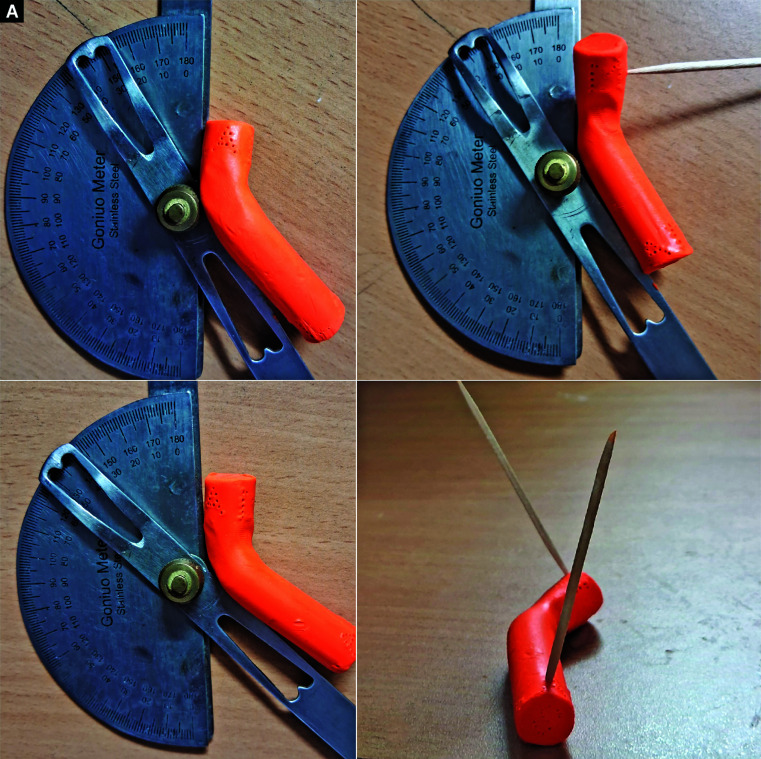
Materials and methods: Using cylinder-shaped non-hardening modelling clay, eight angular (coronal, sagittal and their combinations) and two rotational (internal and external) deformities yielding 16 A-R deformity pairs were simulated for a right-sided model. The magnitudes of A and R deformities were 45° each. Resultant magnitudes of vertical and transverse orientations of the single-cut were constant at 45° and 22.5°, respectively. Transverse rotational orientation of the cut was external for internal rotational deformity and, internal for external rotational deformity. Vertical orientation of the cut was ascending and descending for each of the 32 A-R deformity models. Outcome measure was visual contact between oblique cut surfaces.
Results: After ascending cut and derotational correction, the A-R deformities that maintained contact were varus-internal rotation, procurvatum-internal rotation, varus-procurvatum-internal rotation, varus-recurvatum-internal rotation, valgus-external rotation, recurvatum-external rotation, valgus-recurvatum-external rotation and valgus-procurvatum-external rotation. After descending cut and derotational correction, the A-R deformities that maintained contact were valgus-internal rotation, recurvatum-internal rotation, valgus-recurvatum-internal rotation, valgus-procurvatum-internal rotation, varus-external rotation, procurvatum-external rotation, varus-procurvatum-external rotation and varus-recurvatum-external rotation.
Conclusion: The geometric rules guiding the vertical orientation of single-cut inclined osteotomy in A-R deformity are:Complementary A-R deformity requires an ascending osteotomy.- Varus and/or procurvatum with internal rotation.- Valgus and/or recurvatum with external rotation.Compensatory A-R deformity requires a descending osteotomy.- Varus and/or procurvatum with external rotation.- Valgus and/or recurvatum with internal rotation.In an A-R deformity with dissociative angular components, coronal plane deformity supersedes sagittal plane deformity in dictating the vertical orientation of the osteotomy. This is irrespective of the magnitude of coronal deformity.- Varus-recurvatum with internal or external rotation.- Valgus-procurvatum with internal or external rotation.
Clinical significance: The combination pattern of angular and rotational components (A-R) determines accurate vertical orientation of the cut.Application of the geometric rules bypasses (1) complex calculations, (2) multiple trial-and-error methods and (3) expensive bone models.These simple rules will enable surgeons to consider the appropriate inclined osteotomy for any A-R deformity in clinical practice.The utility of 3D-printed models would be appropriate to improve the precision of the cut before surgery.
How to cite this article: Gopalan B. What is the Geometric Rule that Guides Accurate Vertical Orientation of the Single-cut Inclined Osteotomy in a Combined Angulation-rotation Deformity of Long Bone? Strategies Trauma Limb Reconstr 2025;20(1):11-16.
期刊介绍:
Strategies in Trauma and Limb Reconstruction is dedicated to surgeons, allied medical professionals and researchers in the field of orthopaedics and trauma. The scope of the journal is to discuss the fields of skeletal injury, and the complications thereof, congenital and acquired limb deformities and deficiencies, and orthopaedic-related infection, together with their surgical and non-surgical treatments. The journal publishes original articles, reviews, case reports, descriptions of new or recognised treatment techniques, forum discussions of clinical scenarios and relevant correspondence. It aims to provide a widely accessible source of useful information to practitioners in the field through the problem- or technique-based approach of published articles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


