{"title":"预适应对上消化道肿瘤患者术后预后的影响:荟萃分析。","authors":"Qi Li, Jianhong Liu, Liqing Li, Yeli Luo","doi":"10.1093/bjsopen/zraf091","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of this meta-analysis was to elucidate the effects of prehabilitation (PR) on outcomes after surgery for upper gastrointestinal tract cancer.</p><p><strong>Methods: </strong>PubMed, Web of Science, Embase, and Cochrane databases were searched from inception up to 21 May 2024 for randomized clinical trials (RCTs) and cohort studies investigating PR interventions in patients with upper gastrointestinal tract cancer. Data were synthesized using standardized mean differences (SMDs) and risk ratios (RRs) with corresponding 95% confidence intervals. Sensitivity and subgroup analyses were used to examine the robustness of the results and find possible sources of heterogeneity. Statistical analyses were performed using Review Manager 5.4 and Stata 16.0.</p><p><strong>Results: </strong>Eight RCTs and eight cohort studies were included in the meta-analysis. Compared with the control group (no PR), the PR group had a significantly shorter postoperative length of hospital stay (SMD -0.27; 95% confidence interval (c.i.) -0.47 to -0.07; P = 0.008), a significant reduction in the occurrence of pneumonia after the surgery (RR 0.71; 95% c.i. 0.50 to 1.00; P = 0.005), and a greater improvement in the 6-minute walk distance (SMD 0.95; 95% c.i. 0.68 to 1.22; P < 0.00001). However, there were no significant differences between the control and PR groups in overall postoperative complications, anastomotic leakage, overall pulmonary complications, operative time, intraoperative blood loss, wound infection rate, in-hospital mortality, or recurrence rate (all P > 0.05).</p><p><strong>Conclusion: </strong>For the population with upper gastrointestinal tract cancer, PR can partially lower the risk of postoperative pneumonia and promote faster postoperative recovery. Given the inherent limitations in the included studies, more large-scale RCTs are needed to verify these findings.</p>","PeriodicalId":9028,"journal":{"name":"BJS Open","volume":"9 5","pages":""},"PeriodicalIF":4.5000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12452279/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effect of prehabilitation on postoperative outcomes in patients with upper gastrointestinal tract cancer: meta-analysis.\",\"authors\":\"Qi Li, Jianhong Liu, Liqing Li, Yeli Luo\",\"doi\":\"10.1093/bjsopen/zraf091\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The aim of this meta-analysis was to elucidate the effects of prehabilitation (PR) on outcomes after surgery for upper gastrointestinal tract cancer.</p><p><strong>Methods: </strong>PubMed, Web of Science, Embase, and Cochrane databases were searched from inception up to 21 May 2024 for randomized clinical trials (RCTs) and cohort studies investigating PR interventions in patients with upper gastrointestinal tract cancer. Data were synthesized using standardized mean differences (SMDs) and risk ratios (RRs) with corresponding 95% confidence intervals. Sensitivity and subgroup analyses were used to examine the robustness of the results and find possible sources of heterogeneity. Statistical analyses were performed using Review Manager 5.4 and Stata 16.0.</p><p><strong>Results: </strong>Eight RCTs and eight cohort studies were included in the meta-analysis. Compared with the control group (no PR), the PR group had a significantly shorter postoperative length of hospital stay (SMD -0.27; 95% confidence interval (c.i.) -0.47 to -0.07; P = 0.008), a significant reduction in the occurrence of pneumonia after the surgery (RR 0.71; 95% c.i. 0.50 to 1.00; P = 0.005), and a greater improvement in the 6-minute walk distance (SMD 0.95; 95% c.i. 0.68 to 1.22; P < 0.00001). However, there were no significant differences between the control and PR groups in overall postoperative complications, anastomotic leakage, overall pulmonary complications, operative time, intraoperative blood loss, wound infection rate, in-hospital mortality, or recurrence rate (all P > 0.05).</p><p><strong>Conclusion: </strong>For the population with upper gastrointestinal tract cancer, PR can partially lower the risk of postoperative pneumonia and promote faster postoperative recovery. Given the inherent limitations in the included studies, more large-scale RCTs are needed to verify these findings.</p>\",\"PeriodicalId\":9028,\"journal\":{\"name\":\"BJS Open\",\"volume\":\"9 5\",\"pages\":\"\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2025-09-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12452279/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJS Open\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/bjsopen/zraf091\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJS Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjsopen/zraf091","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
背景:本荟萃分析的目的是阐明预适应(PR)对上消化道肿瘤手术后预后的影响。方法:检索PubMed、Web of Science、Embase和Cochrane数据库,检索从建立到2024年5月21日的随机临床试验(rct)和队列研究,研究PR干预对上胃肠道癌患者的影响。采用标准化平均差异(SMDs)和相应95%置信区间的风险比(rr)综合数据。采用敏感性和亚组分析来检验结果的稳健性,并寻找可能的异质性来源。使用Review Manager 5.4和Stata 16.0进行统计分析。结果:meta分析纳入8项随机对照试验和8项队列研究。与对照组(无PR)相比,PR组术后住院时间明显缩短(SMD -0.27; 95%可信区间(ci . 1)。-0.47 ~ -0.07;P = 0.008),术后肺炎发生率显著降低(RR = 0.71; 95% ci . 0.50 ~ 1.00; P = 0.005), 6分钟步行距离改善更大(SMD = 0.95; 95% ci . 0.68 ~ 1.22; P < 0.00001)。对照组与PR组在术后总并发症、吻合口漏、肺总并发症、手术时间、术中出血量、伤口感染率、住院死亡率、复发率等方面差异均无统计学意义(P < 0.05)。结论:对于上消化道肿瘤患者,PR可部分降低术后肺炎的发生风险,促进术后更快恢复。考虑到纳入研究的固有局限性,需要更多的大规模随机对照试验来验证这些发现。
Effect of prehabilitation on postoperative outcomes in patients with upper gastrointestinal tract cancer: meta-analysis.
Background: The aim of this meta-analysis was to elucidate the effects of prehabilitation (PR) on outcomes after surgery for upper gastrointestinal tract cancer.
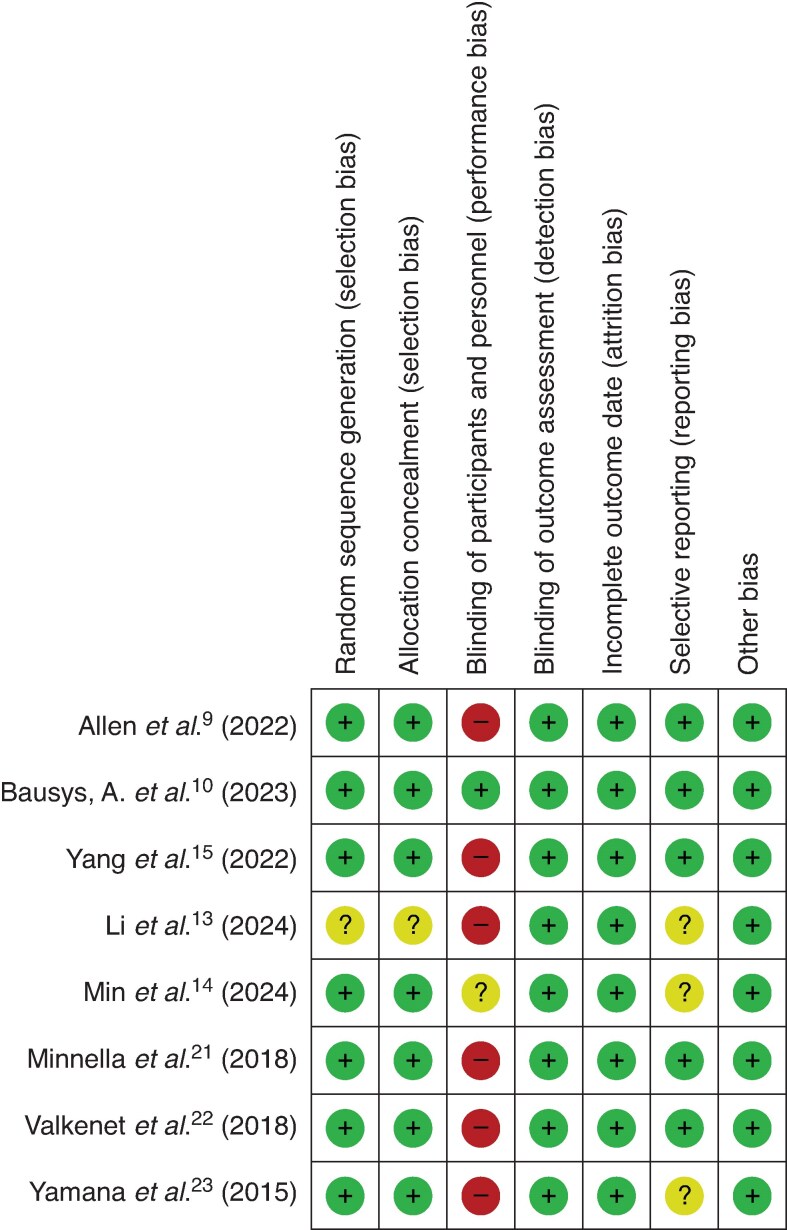
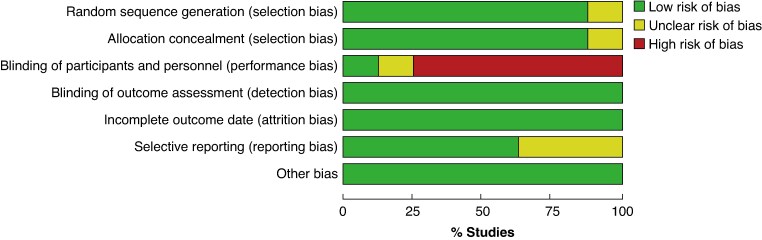
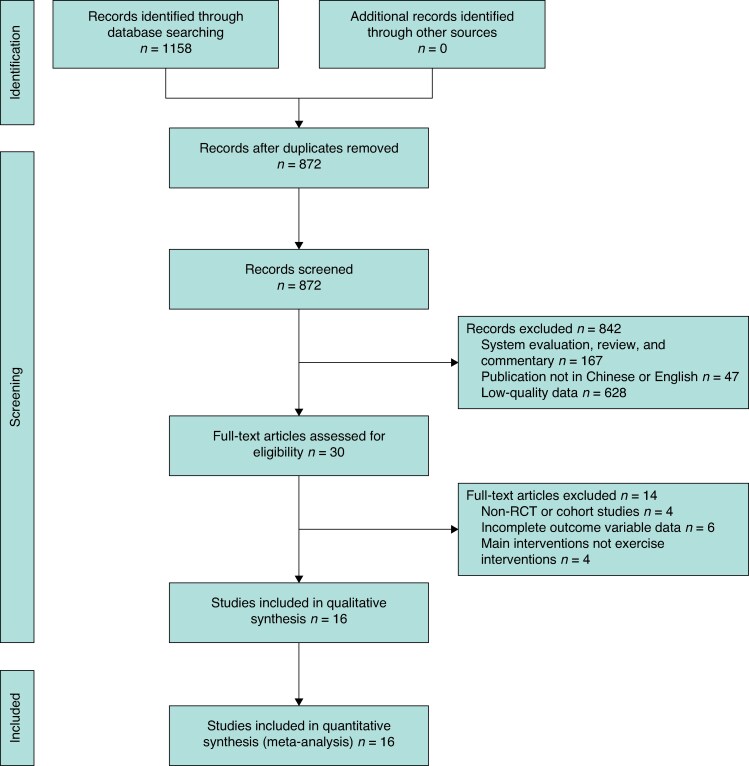
Methods: PubMed, Web of Science, Embase, and Cochrane databases were searched from inception up to 21 May 2024 for randomized clinical trials (RCTs) and cohort studies investigating PR interventions in patients with upper gastrointestinal tract cancer. Data were synthesized using standardized mean differences (SMDs) and risk ratios (RRs) with corresponding 95% confidence intervals. Sensitivity and subgroup analyses were used to examine the robustness of the results and find possible sources of heterogeneity. Statistical analyses were performed using Review Manager 5.4 and Stata 16.0.
Results: Eight RCTs and eight cohort studies were included in the meta-analysis. Compared with the control group (no PR), the PR group had a significantly shorter postoperative length of hospital stay (SMD -0.27; 95% confidence interval (c.i.) -0.47 to -0.07; P = 0.008), a significant reduction in the occurrence of pneumonia after the surgery (RR 0.71; 95% c.i. 0.50 to 1.00; P = 0.005), and a greater improvement in the 6-minute walk distance (SMD 0.95; 95% c.i. 0.68 to 1.22; P < 0.00001). However, there were no significant differences between the control and PR groups in overall postoperative complications, anastomotic leakage, overall pulmonary complications, operative time, intraoperative blood loss, wound infection rate, in-hospital mortality, or recurrence rate (all P > 0.05).
Conclusion: For the population with upper gastrointestinal tract cancer, PR can partially lower the risk of postoperative pneumonia and promote faster postoperative recovery. Given the inherent limitations in the included studies, more large-scale RCTs are needed to verify these findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


