Deirdre J Cohen, Judith D Goldberg, Lawrence Leichman, Tsivia Hochman, Elliot Newman, Kevin Du, Alec Megibow, Paul Oberstein, Raed Al-Rajabi, Aaron J Scott, Tanios Bekaii-Saab, Wells A Messersmith, Colin Weekes
{"title":"可切除和交界性可切除胰腺腺癌的围手术期治疗:一项学术胃肠道癌症协会(AGICC)研究。","authors":"Deirdre J Cohen, Judith D Goldberg, Lawrence Leichman, Tsivia Hochman, Elliot Newman, Kevin Du, Alec Megibow, Paul Oberstein, Raed Al-Rajabi, Aaron J Scott, Tanios Bekaii-Saab, Wells A Messersmith, Colin Weekes","doi":"10.1093/oncolo/oyaf271","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgical resection without visible or residual microscopic disease (R0 resection) is known as the optimal path to cure localized pancreatic cancer (PDAC). Neoadjuvant therapy (NAT) is used to improve R0 resection rates; however, the optimal regimen is unclear. We assessed the safety and efficacy of peri-operative gemcitabine/nab-paclitaxel (GEM/NAB) and pre-operative stereotactic body radiotherapy (SBRT) in patients with resectable (R-PDAC) and borderline resectable PDAC (BR-PDAC).</p><p><strong>Patients and methods: </strong>This was a prospective, multicenter single arm phase 2 study in patients with R-PDAC and BR-PDAC. Patients received three cycles of GEM/NAB prior to SBRT followed by surgery and three cycles of adjuvant GEM/NAB. Primary endpoint was R0 surgical resection rate in each cohort. Secondary endpoints included safety and overall survival (OS).</p><p><strong>Results: </strong>Eighty-six patients consented and following radiologic screening, 49 were enrolled into two cohorts: R-PDAC (n = 20) and BR-PDAC (n = 29) between June 2016 and April 2021. Seventy percent of R-PDAC (14/20) and 55.2% of BR-PDAC patients (16/29) completed all NAT. Eleven R-PDAC (55.0%) and 11 BR-PDAC patients (37.9%) underwent surgical resection. Nine R-PDAC (45.0%) and 9 BR-PDAC patients (31.0%) had R0 resections. The median OS for R-PDAC and BR-PDAC patients with R0 resections was 22 months (95% CI: 17.7 months-NA) and 39 months (95%CI: 13.21 months-NA), respectively.</p><p><strong>Conclusion: </strong>While the trial failed to meet one of its primary objectives as only 45% of R-PDAC patients had an R0 resection, the objective of 30% R0 resection for the BR-PDAC group was met. NAT should be part of current therapeutic strategies for BR-PDAC; however, our trial does not answer what is the best NAT for BR-PDAC.</p><p><strong>Trial registration: </strong>NCT02723331.</p>","PeriodicalId":54686,"journal":{"name":"Oncologist","volume":" ","pages":""},"PeriodicalIF":4.2000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12526980/pdf/","citationCount":"0","resultStr":"{\"title\":\"Perioperative therapy for resectable and borderline resectable pancreatic adenocarcinoma: an Academic Gastrointestinal Cancer Consortium Study.\",\"authors\":\"Deirdre J Cohen, Judith D Goldberg, Lawrence Leichman, Tsivia Hochman, Elliot Newman, Kevin Du, Alec Megibow, Paul Oberstein, Raed Al-Rajabi, Aaron J Scott, Tanios Bekaii-Saab, Wells A Messersmith, Colin Weekes\",\"doi\":\"10.1093/oncolo/oyaf271\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Surgical resection without visible or residual microscopic disease (R0 resection) is known as the optimal path to cure localized pancreatic cancer (PDAC). Neoadjuvant therapy (NAT) is used to improve R0 resection rates; however, the optimal regimen is unclear. We assessed the safety and efficacy of peri-operative gemcitabine/nab-paclitaxel (GEM/NAB) and pre-operative stereotactic body radiotherapy (SBRT) in patients with resectable (R-PDAC) and borderline resectable PDAC (BR-PDAC).</p><p><strong>Patients and methods: </strong>This was a prospective, multicenter single arm phase 2 study in patients with R-PDAC and BR-PDAC. Patients received three cycles of GEM/NAB prior to SBRT followed by surgery and three cycles of adjuvant GEM/NAB. Primary endpoint was R0 surgical resection rate in each cohort. Secondary endpoints included safety and overall survival (OS).</p><p><strong>Results: </strong>Eighty-six patients consented and following radiologic screening, 49 were enrolled into two cohorts: R-PDAC (n = 20) and BR-PDAC (n = 29) between June 2016 and April 2021. Seventy percent of R-PDAC (14/20) and 55.2% of BR-PDAC patients (16/29) completed all NAT. Eleven R-PDAC (55.0%) and 11 BR-PDAC patients (37.9%) underwent surgical resection. Nine R-PDAC (45.0%) and 9 BR-PDAC patients (31.0%) had R0 resections. The median OS for R-PDAC and BR-PDAC patients with R0 resections was 22 months (95% CI: 17.7 months-NA) and 39 months (95%CI: 13.21 months-NA), respectively.</p><p><strong>Conclusion: </strong>While the trial failed to meet one of its primary objectives as only 45% of R-PDAC patients had an R0 resection, the objective of 30% R0 resection for the BR-PDAC group was met. NAT should be part of current therapeutic strategies for BR-PDAC; however, our trial does not answer what is the best NAT for BR-PDAC.</p><p><strong>Trial registration: </strong>NCT02723331.</p>\",\"PeriodicalId\":54686,\"journal\":{\"name\":\"Oncologist\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":4.2000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12526980/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Oncologist\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/oncolo/oyaf271\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Oncologist","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/oncolo/oyaf271","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Perioperative therapy for resectable and borderline resectable pancreatic adenocarcinoma: an Academic Gastrointestinal Cancer Consortium Study.
Background: Surgical resection without visible or residual microscopic disease (R0 resection) is known as the optimal path to cure localized pancreatic cancer (PDAC). Neoadjuvant therapy (NAT) is used to improve R0 resection rates; however, the optimal regimen is unclear. We assessed the safety and efficacy of peri-operative gemcitabine/nab-paclitaxel (GEM/NAB) and pre-operative stereotactic body radiotherapy (SBRT) in patients with resectable (R-PDAC) and borderline resectable PDAC (BR-PDAC).
Patients and methods: This was a prospective, multicenter single arm phase 2 study in patients with R-PDAC and BR-PDAC. Patients received three cycles of GEM/NAB prior to SBRT followed by surgery and three cycles of adjuvant GEM/NAB. Primary endpoint was R0 surgical resection rate in each cohort. Secondary endpoints included safety and overall survival (OS).
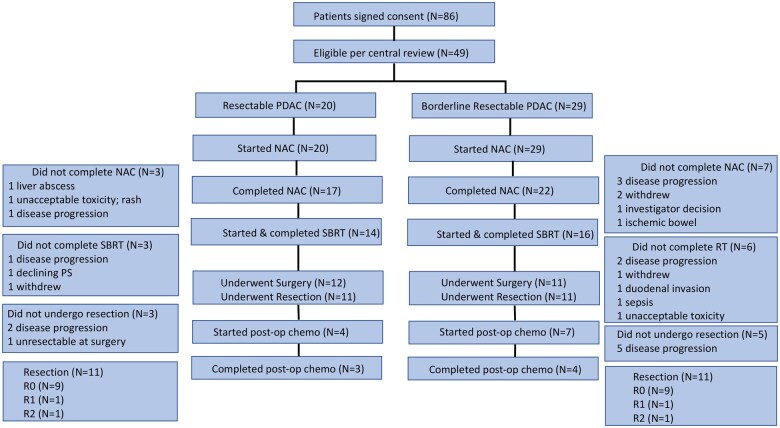
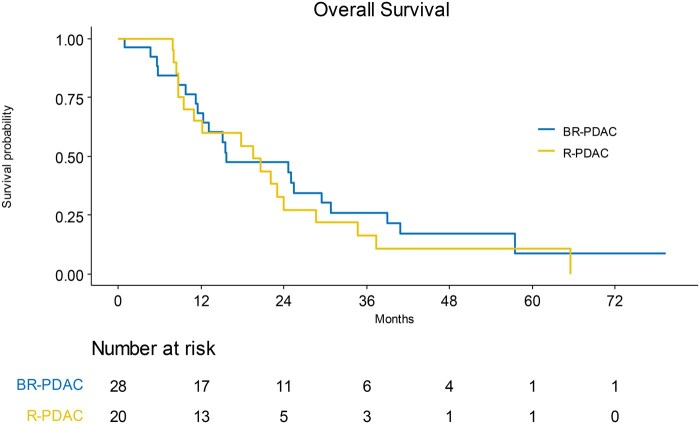
Results: Eighty-six patients consented and following radiologic screening, 49 were enrolled into two cohorts: R-PDAC (n = 20) and BR-PDAC (n = 29) between June 2016 and April 2021. Seventy percent of R-PDAC (14/20) and 55.2% of BR-PDAC patients (16/29) completed all NAT. Eleven R-PDAC (55.0%) and 11 BR-PDAC patients (37.9%) underwent surgical resection. Nine R-PDAC (45.0%) and 9 BR-PDAC patients (31.0%) had R0 resections. The median OS for R-PDAC and BR-PDAC patients with R0 resections was 22 months (95% CI: 17.7 months-NA) and 39 months (95%CI: 13.21 months-NA), respectively.
Conclusion: While the trial failed to meet one of its primary objectives as only 45% of R-PDAC patients had an R0 resection, the objective of 30% R0 resection for the BR-PDAC group was met. NAT should be part of current therapeutic strategies for BR-PDAC; however, our trial does not answer what is the best NAT for BR-PDAC.
期刊介绍:
The Oncologist® is dedicated to translating the latest research developments into the best multidimensional care for cancer patients. Thus, The Oncologist is committed to helping physicians excel in this ever-expanding environment through the publication of timely reviews, original studies, and commentaries on important developments. We believe that the practice of oncology requires both an understanding of a range of disciplines encompassing basic science related to cancer, translational research, and clinical practice, but also the socioeconomic and psychosocial factors that determine access to care and quality of life and function following cancer treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


