Muhammad Usman Almani, Rasha Khan, Noor Fatima, Muhammad Yousuf, Aman Amanullah
{"title":"三尖瓣反流对心力衰竭患者临床预后的影响。","authors":"Muhammad Usman Almani, Rasha Khan, Noor Fatima, Muhammad Yousuf, Aman Amanullah","doi":"10.1002/puh2.70092","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tricuspid regurgitation (TR) is a common occurrence in patients with heart failure (HF), and its role in disease progression has gained attention in recent years. Although TR can worsen clinical outcomes in HF patients, the impact of gender, racial, and socioeconomic factors remains largely unexplored. With growing evidence supporting the role of percutaneous interventions for the treatment of significant TR, understanding these disparities is more crucial than ever.</p><p><strong>Methods: </strong>Data were extracted from the National Inpatient and National Readmission 2016-2020 Databases. We used ICD-10 code I50 to identify the patients primarily admitted for HF and subdivided the cohort into two groups based on the presence or absence of TR. We performed multivariable logistic regression analysis to determine odds of the in-hospital mortality and multivariable Cox regression analysis to assess the 30- and 90-day hospital readmission in HF patients with and without TR. All the analyses were adjusted for age, gender, insurance status, Charlson comorbidity index, and hospital characteristics. STATA 16 software was used for analysis.</p><p><strong>Results: </strong>There was no difference in the in-hospital mortality among HF patients with and without TR (OR: 1.04, 95% CI 0.94-1.16, <i>p</i> = 0.442) except in certain subgroups of HF patients. HF patients with TR were 6% more likely to have HF-specific readmission in 30 days (HR: 1.06, 95% CI 1.00-1.13, <i>p</i> = 0.044) and 9% more likely to have HF-specific readmission in 90 days (HR: 1.09, 95% CI 1.03-1.15, <i>p</i> = 0.002). Subgroup analysis revealed significant gender, racial, and socioeconomic disparities in the in-hospital mortality and the readmission outcomes of HF patients with TR compared to those without TR.</p><p><strong>Conclusion: </strong>In our population-based survey analysis, we observed significant gender, racial, and socioeconomic disparities in the clinical outcomes of HF patients with TR compared to those without TR.</p>","PeriodicalId":74613,"journal":{"name":"Public health challenges","volume":"4 3","pages":"e70092"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12442787/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of Tricuspid Regurgitation on the Clinical Outcomes of Patients with Heart Failure.\",\"authors\":\"Muhammad Usman Almani, Rasha Khan, Noor Fatima, Muhammad Yousuf, Aman Amanullah\",\"doi\":\"10.1002/puh2.70092\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Tricuspid regurgitation (TR) is a common occurrence in patients with heart failure (HF), and its role in disease progression has gained attention in recent years. Although TR can worsen clinical outcomes in HF patients, the impact of gender, racial, and socioeconomic factors remains largely unexplored. With growing evidence supporting the role of percutaneous interventions for the treatment of significant TR, understanding these disparities is more crucial than ever.</p><p><strong>Methods: </strong>Data were extracted from the National Inpatient and National Readmission 2016-2020 Databases. We used ICD-10 code I50 to identify the patients primarily admitted for HF and subdivided the cohort into two groups based on the presence or absence of TR. We performed multivariable logistic regression analysis to determine odds of the in-hospital mortality and multivariable Cox regression analysis to assess the 30- and 90-day hospital readmission in HF patients with and without TR. All the analyses were adjusted for age, gender, insurance status, Charlson comorbidity index, and hospital characteristics. STATA 16 software was used for analysis.</p><p><strong>Results: </strong>There was no difference in the in-hospital mortality among HF patients with and without TR (OR: 1.04, 95% CI 0.94-1.16, <i>p</i> = 0.442) except in certain subgroups of HF patients. HF patients with TR were 6% more likely to have HF-specific readmission in 30 days (HR: 1.06, 95% CI 1.00-1.13, <i>p</i> = 0.044) and 9% more likely to have HF-specific readmission in 90 days (HR: 1.09, 95% CI 1.03-1.15, <i>p</i> = 0.002). Subgroup analysis revealed significant gender, racial, and socioeconomic disparities in the in-hospital mortality and the readmission outcomes of HF patients with TR compared to those without TR.</p><p><strong>Conclusion: </strong>In our population-based survey analysis, we observed significant gender, racial, and socioeconomic disparities in the clinical outcomes of HF patients with TR compared to those without TR.</p>\",\"PeriodicalId\":74613,\"journal\":{\"name\":\"Public health challenges\",\"volume\":\"4 3\",\"pages\":\"e70092\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12442787/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Public health challenges\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/puh2.70092\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Public health challenges","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/puh2.70092","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:三尖瓣反流(TR)是心力衰竭(HF)患者的常见现象,近年来其在疾病进展中的作用已引起人们的关注。虽然TR可使心衰患者的临床结果恶化,但性别、种族和社会经济因素的影响在很大程度上仍未得到研究。随着越来越多的证据支持经皮介入治疗严重TR的作用,了解这些差异比以往任何时候都更加重要。方法:数据提取自2016-2020年国家住院和国家再入院数据库。我们使用ICD-10代码I50识别主要因HF入院的患者,并根据是否存在TR将队列细分为两组。我们进行了多变量logistic回归分析以确定住院死亡率的几率,并进行了多变量Cox回归分析以评估有TR和无TR的HF患者的30天和90天再入院率。所有分析均根据年龄、性别、保险状况、Charlson合并症指数、医院的特点。采用STATA 16软件进行分析。结果:除了HF患者的某些亚组外,合并和不合并TR的HF患者的住院死亡率无差异(OR: 1.04, 95% CI 0.94-1.16, p = 0.442)。合并TR的HF患者在30天内发生HF特异性再入院的可能性增加6% (HR: 1.06, 95% CI 1.00-1.13, p = 0.044),在90天内发生HF特异性再入院的可能性增加9% (HR: 1.09, 95% CI 1.03-1.15, p = 0.002)。亚组分析显示,与没有TR的患者相比,合并TR的HF患者的住院死亡率和再入院结果存在显著的性别、种族和社会经济差异。结论:在我们基于人群的调查分析中,我们观察到合并TR的HF患者的临床结果与没有TR的患者相比存在显著的性别、种族和社会经济差异。
Impact of Tricuspid Regurgitation on the Clinical Outcomes of Patients with Heart Failure.
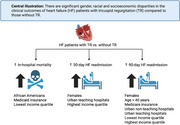
Background: Tricuspid regurgitation (TR) is a common occurrence in patients with heart failure (HF), and its role in disease progression has gained attention in recent years. Although TR can worsen clinical outcomes in HF patients, the impact of gender, racial, and socioeconomic factors remains largely unexplored. With growing evidence supporting the role of percutaneous interventions for the treatment of significant TR, understanding these disparities is more crucial than ever.
Methods: Data were extracted from the National Inpatient and National Readmission 2016-2020 Databases. We used ICD-10 code I50 to identify the patients primarily admitted for HF and subdivided the cohort into two groups based on the presence or absence of TR. We performed multivariable logistic regression analysis to determine odds of the in-hospital mortality and multivariable Cox regression analysis to assess the 30- and 90-day hospital readmission in HF patients with and without TR. All the analyses were adjusted for age, gender, insurance status, Charlson comorbidity index, and hospital characteristics. STATA 16 software was used for analysis.
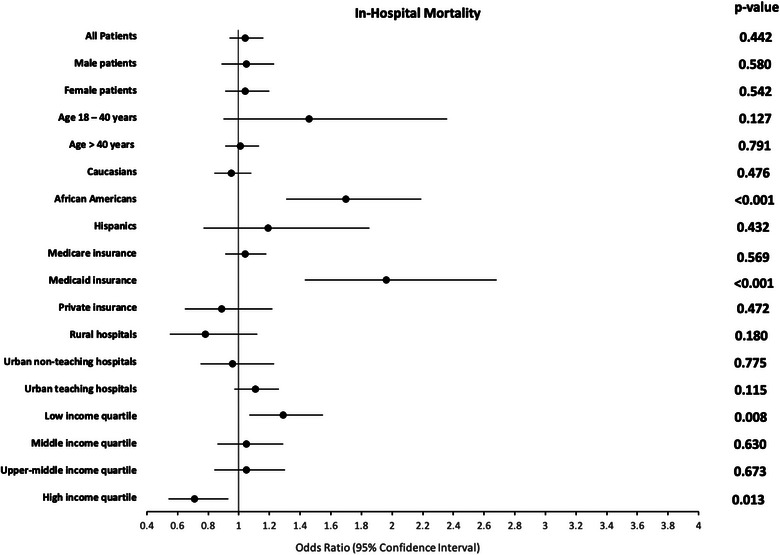
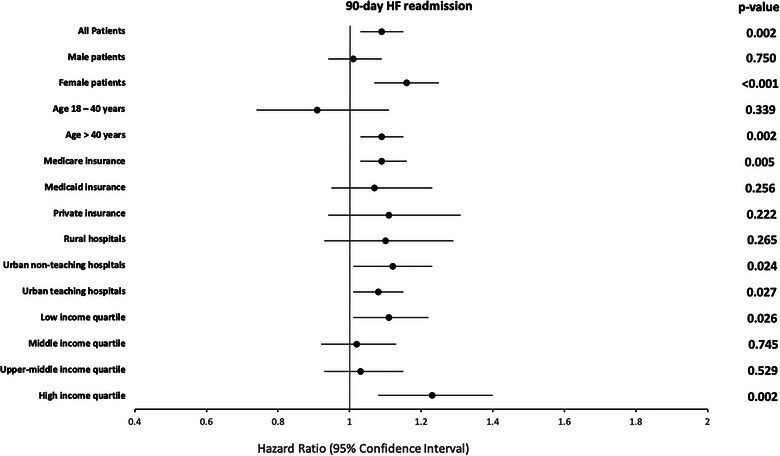
Results: There was no difference in the in-hospital mortality among HF patients with and without TR (OR: 1.04, 95% CI 0.94-1.16, p = 0.442) except in certain subgroups of HF patients. HF patients with TR were 6% more likely to have HF-specific readmission in 30 days (HR: 1.06, 95% CI 1.00-1.13, p = 0.044) and 9% more likely to have HF-specific readmission in 90 days (HR: 1.09, 95% CI 1.03-1.15, p = 0.002). Subgroup analysis revealed significant gender, racial, and socioeconomic disparities in the in-hospital mortality and the readmission outcomes of HF patients with TR compared to those without TR.
Conclusion: In our population-based survey analysis, we observed significant gender, racial, and socioeconomic disparities in the clinical outcomes of HF patients with TR compared to those without TR.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


