Ahad Mahmud Khan, Md Shafiqul Islam, Nabidul Haque Chowdhury, Salahuddin Ahmed, Rezwana Tabassum, Sadia Afrin, Zannatul Ferdush Amin, Kazi Sazzadul Haque, Afroza Yeasmin Rumi, Jawata Rahman, Rakib Bhuiyan, Rizouan Ur Rashid, Kamrun Nahar, Robynne Simpson, Ayaz Ahmed, Md Mozibur Rahman, Ting Shi, Abdullah H Baqui, Steve Cunningham, Eric D McCollum, Harry Campbell
{"title":"使用参考视频专家小组评估自动呼吸频率计数器检测儿童呼吸急促肺炎的性能。","authors":"Ahad Mahmud Khan, Md Shafiqul Islam, Nabidul Haque Chowdhury, Salahuddin Ahmed, Rezwana Tabassum, Sadia Afrin, Zannatul Ferdush Amin, Kazi Sazzadul Haque, Afroza Yeasmin Rumi, Jawata Rahman, Rakib Bhuiyan, Rizouan Ur Rashid, Kamrun Nahar, Robynne Simpson, Ayaz Ahmed, Md Mozibur Rahman, Ting Shi, Abdullah H Baqui, Steve Cunningham, Eric D McCollum, Harry Campbell","doi":"10.1186/s44247-025-00175-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>According to the World Health Organization's Integrated Management of Childhood Illness (IMCI) guidelines, childhood pneumonia diagnosis relies on counting respiratory rate (RR). Counting RR by health workers is frequently inaccurate, leading to misdiagnosis and poor outcomes. Automated RR counters could potentially overcome these limitations. To address this gap, we introduced an automated RR counter and developed a reference video expert panel (VEP) to evaluate its performance.</p><p><strong>Methods: </strong>We conducted a cross-sectional study involving children aged 0-59 months with suspected pneumonia in Bangladesh. The RR of children was counted using an automated counter (ChARM) and chest movements were simultaneously videotaped. These videos were interpreted by the VEP, trained to a standard procedure. We assessed ChARM's accuracy in comparison to the RR generated by the VEP and summarised the time taken to count RR by ChARM.</p><p><strong>Results: </strong>Among 339 enrolled children, ChARM successfully counted the RR of 294 children (86.7%). The VEP reached a consensus (i.e., RR count difference within two breaths per minute (bpm) between two VEP members) in 257 of the 294 children (87.4%). ChARM and the VEP agreed on RR counts within two bpm in 68.1% of children (<i>n</i> = 175/257), with a mean difference of 1.7 bpm and limits of agreement ranging from -6.7 to 10.2 bpm. ChARM classified age-adjusted fast and normal breathing with a sensitivity of 95.8% (95% CI: 88.1-99.1) and a specificity of 93.5% (95% CI: 89.0-96.6), demonstrating high agreement (kappa = 0.86). The median time to count the RR by ChARM was 66 s (interquartile range: 61-73 s).</p><p><strong>Conclusions: </strong>ChARM counted RR accurately against a VEP reference, indicating a potential role in supporting health workers to diagnose pneumonia. However, it was unsuccessful for 1 in 8 cases, typically those more clinically challenging, suggesting a possible systematic bias. Further research is needed to address these issues and confirm ChARM's reliability for broader use in real-world settings.</p><p><strong>Trial registration: </strong>Current Controlled Trials ISRCTN14120515, registered retrospectively on 19 September 2024.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1186/s44247-025-00175-3.</p>","PeriodicalId":72426,"journal":{"name":"BMC digital health","volume":"3 1","pages":"32"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12442458/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluating the performance of an automated respiratory rate counter in detecting fast breathing pneumonia in children using a reference video expert panel.\",\"authors\":\"Ahad Mahmud Khan, Md Shafiqul Islam, Nabidul Haque Chowdhury, Salahuddin Ahmed, Rezwana Tabassum, Sadia Afrin, Zannatul Ferdush Amin, Kazi Sazzadul Haque, Afroza Yeasmin Rumi, Jawata Rahman, Rakib Bhuiyan, Rizouan Ur Rashid, Kamrun Nahar, Robynne Simpson, Ayaz Ahmed, Md Mozibur Rahman, Ting Shi, Abdullah H Baqui, Steve Cunningham, Eric D McCollum, Harry Campbell\",\"doi\":\"10.1186/s44247-025-00175-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>According to the World Health Organization's Integrated Management of Childhood Illness (IMCI) guidelines, childhood pneumonia diagnosis relies on counting respiratory rate (RR). Counting RR by health workers is frequently inaccurate, leading to misdiagnosis and poor outcomes. Automated RR counters could potentially overcome these limitations. To address this gap, we introduced an automated RR counter and developed a reference video expert panel (VEP) to evaluate its performance.</p><p><strong>Methods: </strong>We conducted a cross-sectional study involving children aged 0-59 months with suspected pneumonia in Bangladesh. The RR of children was counted using an automated counter (ChARM) and chest movements were simultaneously videotaped. These videos were interpreted by the VEP, trained to a standard procedure. We assessed ChARM's accuracy in comparison to the RR generated by the VEP and summarised the time taken to count RR by ChARM.</p><p><strong>Results: </strong>Among 339 enrolled children, ChARM successfully counted the RR of 294 children (86.7%). The VEP reached a consensus (i.e., RR count difference within two breaths per minute (bpm) between two VEP members) in 257 of the 294 children (87.4%). ChARM and the VEP agreed on RR counts within two bpm in 68.1% of children (<i>n</i> = 175/257), with a mean difference of 1.7 bpm and limits of agreement ranging from -6.7 to 10.2 bpm. ChARM classified age-adjusted fast and normal breathing with a sensitivity of 95.8% (95% CI: 88.1-99.1) and a specificity of 93.5% (95% CI: 89.0-96.6), demonstrating high agreement (kappa = 0.86). The median time to count the RR by ChARM was 66 s (interquartile range: 61-73 s).</p><p><strong>Conclusions: </strong>ChARM counted RR accurately against a VEP reference, indicating a potential role in supporting health workers to diagnose pneumonia. However, it was unsuccessful for 1 in 8 cases, typically those more clinically challenging, suggesting a possible systematic bias. Further research is needed to address these issues and confirm ChARM's reliability for broader use in real-world settings.</p><p><strong>Trial registration: </strong>Current Controlled Trials ISRCTN14120515, registered retrospectively on 19 September 2024.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1186/s44247-025-00175-3.</p>\",\"PeriodicalId\":72426,\"journal\":{\"name\":\"BMC digital health\",\"volume\":\"3 1\",\"pages\":\"32\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12442458/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC digital health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44247-025-00175-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44247-025-00175-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Evaluating the performance of an automated respiratory rate counter in detecting fast breathing pneumonia in children using a reference video expert panel.
Background: According to the World Health Organization's Integrated Management of Childhood Illness (IMCI) guidelines, childhood pneumonia diagnosis relies on counting respiratory rate (RR). Counting RR by health workers is frequently inaccurate, leading to misdiagnosis and poor outcomes. Automated RR counters could potentially overcome these limitations. To address this gap, we introduced an automated RR counter and developed a reference video expert panel (VEP) to evaluate its performance.
Methods: We conducted a cross-sectional study involving children aged 0-59 months with suspected pneumonia in Bangladesh. The RR of children was counted using an automated counter (ChARM) and chest movements were simultaneously videotaped. These videos were interpreted by the VEP, trained to a standard procedure. We assessed ChARM's accuracy in comparison to the RR generated by the VEP and summarised the time taken to count RR by ChARM.
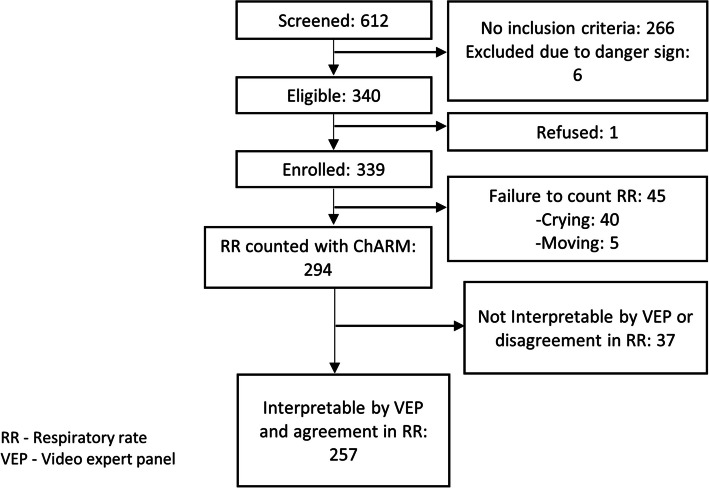
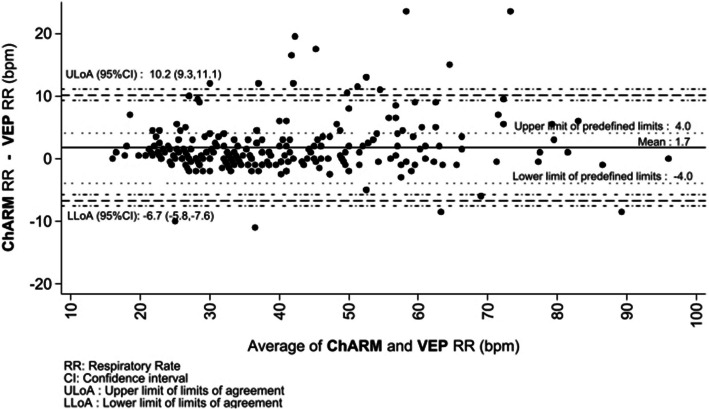
Results: Among 339 enrolled children, ChARM successfully counted the RR of 294 children (86.7%). The VEP reached a consensus (i.e., RR count difference within two breaths per minute (bpm) between two VEP members) in 257 of the 294 children (87.4%). ChARM and the VEP agreed on RR counts within two bpm in 68.1% of children (n = 175/257), with a mean difference of 1.7 bpm and limits of agreement ranging from -6.7 to 10.2 bpm. ChARM classified age-adjusted fast and normal breathing with a sensitivity of 95.8% (95% CI: 88.1-99.1) and a specificity of 93.5% (95% CI: 89.0-96.6), demonstrating high agreement (kappa = 0.86). The median time to count the RR by ChARM was 66 s (interquartile range: 61-73 s).
Conclusions: ChARM counted RR accurately against a VEP reference, indicating a potential role in supporting health workers to diagnose pneumonia. However, it was unsuccessful for 1 in 8 cases, typically those more clinically challenging, suggesting a possible systematic bias. Further research is needed to address these issues and confirm ChARM's reliability for broader use in real-world settings.
Trial registration: Current Controlled Trials ISRCTN14120515, registered retrospectively on 19 September 2024.
Supplementary information: The online version contains supplementary material available at 10.1186/s44247-025-00175-3.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


