Emily M Becker-Haimes, David S Mandell, Patty B Kuo, Kevin G Lynch, Megan Brady, Sophia Young, Torrey A Creed
{"title":"行为推动提高远程医疗会议的保真度(益处):开发和试点测试远程医疗工具以改善认知行为治疗实施的协议。","authors":"Emily M Becker-Haimes, David S Mandell, Patty B Kuo, Kevin G Lynch, Megan Brady, Sophia Young, Torrey A Creed","doi":"10.2196/76035","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The rapid expansion of telehealth provides a unique opportunity to integrate behavioral economics (BE) strategies into telehealth platforms to improve clinician fidelity to cognitive behavioral therapy (CBT)-either by enhancing clinicians' motivation to use CBT or by helping clinicians who are already motivated to act consistently on their intentions.</p><p><strong>Objective: </strong>We will develop and evaluate \"Tele-BE,\" a novel telehealth platform designed to nudge and incentivize clinicians to use core structural components of CBT. We focus on these structural components because they align with practices most likely to benefit from BE strategies, are delivered across diagnoses, and represent CBT competencies independently linked to improved patient outcomes.</p><p><strong>Methods: </strong>We will refine the Tele-BE prototype in collaboration with clinicians and supervisors, who are the target end users (aim 1). Working closely with our web development team, we will field test and iteratively refine Tele-BE using rapid-cycle prototyping to optimize user experience and fine-tune the BE strategies (aim 2). The revised platform will then be evaluated in a 12-week open trial involving 30 community mental health clinicians, who will be randomized to either Tele-BE or telehealth as usual. Each clinician will deliver treatment to 2 patients, resulting in a total of 60 patient participants. All sessions will be recorded and coded to assess CBT fidelity. Clinicians and patients will complete questionnaires at weeks 1, 5, 9, and 12, with qualitative interviews conducted at the end of the trial. Primary outcomes will focus on fidelity to CBT structural components, measured via coding of recorded sessions. Secondary outcomes will include target implementation mechanisms-intentions and their determinants (attitudes, norms, and self-efficacy)-assessed using mixed methods, as well as overall CBT fidelity (aim 3). Additionally, trial data will be used to evaluate the acceptability and feasibility of Tele-BE from both patient and clinician perspectives, along with any potential ethical concerns associated with its use (aim 4).</p><p><strong>Results: </strong>The study received National Institute of Mental Health funding in June 2024. Recruitment for aim 1 began in October 2024. As of March 2025, 6 participants had been enrolled in the initial development stage. Recruitment is ongoing, and we anticipate completing aim 1 by May 2025, after which we will prepare for aim 2 activities. We aim to complete all study data collection by the end of 2026. In accordance with our grant award, deidentified data from aims 3 and 4 will be submitted to the National Institute of Mental Health Data Archive for participants who consent to data sharing.</p><p><strong>Conclusions: </strong>Findings will provide insight into the utility of a BE-informed telehealth platform for increasing clinicians' use of core structural CBT components, thereby improving overall CBT fidelity and patient outcomes. Results will also inform the design of future confirmatory trials.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT06601062; https://clinicaltrials.gov/ct2/show/NCT06601062.</p><p><strong>International registered report identifier (irrid): </strong>DERR1-10.2196/76035.</p>","PeriodicalId":14755,"journal":{"name":"JMIR Research Protocols","volume":"14 ","pages":"e76035"},"PeriodicalIF":1.5000,"publicationDate":"2025-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12491885/pdf/","citationCount":"0","resultStr":"{\"title\":\"Behavioral Nudges to Enhance Fidelity in Telehealth Sessions (BENEFITS): Protocol for Developing and Pilot Testing a Telehealth Tool to Improve Cognitive Behavioral Therapy Implementation.\",\"authors\":\"Emily M Becker-Haimes, David S Mandell, Patty B Kuo, Kevin G Lynch, Megan Brady, Sophia Young, Torrey A Creed\",\"doi\":\"10.2196/76035\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The rapid expansion of telehealth provides a unique opportunity to integrate behavioral economics (BE) strategies into telehealth platforms to improve clinician fidelity to cognitive behavioral therapy (CBT)-either by enhancing clinicians' motivation to use CBT or by helping clinicians who are already motivated to act consistently on their intentions.</p><p><strong>Objective: </strong>We will develop and evaluate \\\"Tele-BE,\\\" a novel telehealth platform designed to nudge and incentivize clinicians to use core structural components of CBT. We focus on these structural components because they align with practices most likely to benefit from BE strategies, are delivered across diagnoses, and represent CBT competencies independently linked to improved patient outcomes.</p><p><strong>Methods: </strong>We will refine the Tele-BE prototype in collaboration with clinicians and supervisors, who are the target end users (aim 1). Working closely with our web development team, we will field test and iteratively refine Tele-BE using rapid-cycle prototyping to optimize user experience and fine-tune the BE strategies (aim 2). The revised platform will then be evaluated in a 12-week open trial involving 30 community mental health clinicians, who will be randomized to either Tele-BE or telehealth as usual. Each clinician will deliver treatment to 2 patients, resulting in a total of 60 patient participants. All sessions will be recorded and coded to assess CBT fidelity. Clinicians and patients will complete questionnaires at weeks 1, 5, 9, and 12, with qualitative interviews conducted at the end of the trial. Primary outcomes will focus on fidelity to CBT structural components, measured via coding of recorded sessions. Secondary outcomes will include target implementation mechanisms-intentions and their determinants (attitudes, norms, and self-efficacy)-assessed using mixed methods, as well as overall CBT fidelity (aim 3). Additionally, trial data will be used to evaluate the acceptability and feasibility of Tele-BE from both patient and clinician perspectives, along with any potential ethical concerns associated with its use (aim 4).</p><p><strong>Results: </strong>The study received National Institute of Mental Health funding in June 2024. Recruitment for aim 1 began in October 2024. As of March 2025, 6 participants had been enrolled in the initial development stage. Recruitment is ongoing, and we anticipate completing aim 1 by May 2025, after which we will prepare for aim 2 activities. We aim to complete all study data collection by the end of 2026. In accordance with our grant award, deidentified data from aims 3 and 4 will be submitted to the National Institute of Mental Health Data Archive for participants who consent to data sharing.</p><p><strong>Conclusions: </strong>Findings will provide insight into the utility of a BE-informed telehealth platform for increasing clinicians' use of core structural CBT components, thereby improving overall CBT fidelity and patient outcomes. Results will also inform the design of future confirmatory trials.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT06601062; https://clinicaltrials.gov/ct2/show/NCT06601062.</p><p><strong>International registered report identifier (irrid): </strong>DERR1-10.2196/76035.</p>\",\"PeriodicalId\":14755,\"journal\":{\"name\":\"JMIR Research Protocols\",\"volume\":\"14 \",\"pages\":\"e76035\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12491885/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR Research Protocols\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/76035\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Research Protocols","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/76035","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Behavioral Nudges to Enhance Fidelity in Telehealth Sessions (BENEFITS): Protocol for Developing and Pilot Testing a Telehealth Tool to Improve Cognitive Behavioral Therapy Implementation.
Background: The rapid expansion of telehealth provides a unique opportunity to integrate behavioral economics (BE) strategies into telehealth platforms to improve clinician fidelity to cognitive behavioral therapy (CBT)-either by enhancing clinicians' motivation to use CBT or by helping clinicians who are already motivated to act consistently on their intentions.
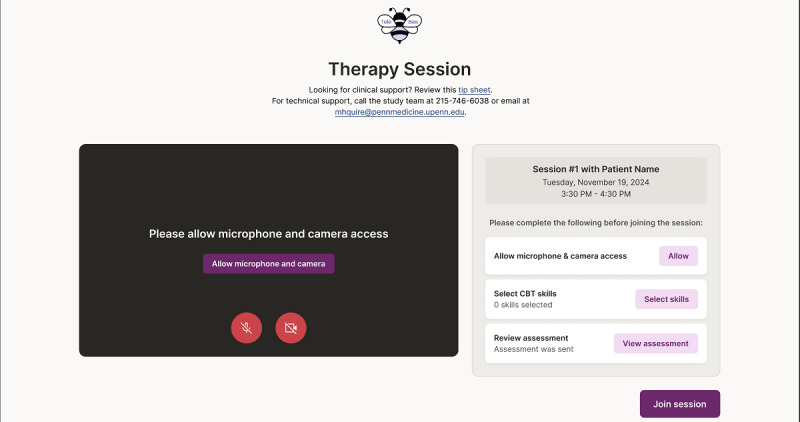
Objective: We will develop and evaluate "Tele-BE," a novel telehealth platform designed to nudge and incentivize clinicians to use core structural components of CBT. We focus on these structural components because they align with practices most likely to benefit from BE strategies, are delivered across diagnoses, and represent CBT competencies independently linked to improved patient outcomes.
Methods: We will refine the Tele-BE prototype in collaboration with clinicians and supervisors, who are the target end users (aim 1). Working closely with our web development team, we will field test and iteratively refine Tele-BE using rapid-cycle prototyping to optimize user experience and fine-tune the BE strategies (aim 2). The revised platform will then be evaluated in a 12-week open trial involving 30 community mental health clinicians, who will be randomized to either Tele-BE or telehealth as usual. Each clinician will deliver treatment to 2 patients, resulting in a total of 60 patient participants. All sessions will be recorded and coded to assess CBT fidelity. Clinicians and patients will complete questionnaires at weeks 1, 5, 9, and 12, with qualitative interviews conducted at the end of the trial. Primary outcomes will focus on fidelity to CBT structural components, measured via coding of recorded sessions. Secondary outcomes will include target implementation mechanisms-intentions and their determinants (attitudes, norms, and self-efficacy)-assessed using mixed methods, as well as overall CBT fidelity (aim 3). Additionally, trial data will be used to evaluate the acceptability and feasibility of Tele-BE from both patient and clinician perspectives, along with any potential ethical concerns associated with its use (aim 4).
Results: The study received National Institute of Mental Health funding in June 2024. Recruitment for aim 1 began in October 2024. As of March 2025, 6 participants had been enrolled in the initial development stage. Recruitment is ongoing, and we anticipate completing aim 1 by May 2025, after which we will prepare for aim 2 activities. We aim to complete all study data collection by the end of 2026. In accordance with our grant award, deidentified data from aims 3 and 4 will be submitted to the National Institute of Mental Health Data Archive for participants who consent to data sharing.
Conclusions: Findings will provide insight into the utility of a BE-informed telehealth platform for increasing clinicians' use of core structural CBT components, thereby improving overall CBT fidelity and patient outcomes. Results will also inform the design of future confirmatory trials.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


