{"title":"诺伍德手术治疗左心发育不全综合征和变异新生儿11年的单中心经验。","authors":"Akihiro Nakamura, Yuichi Ishikawa","doi":"10.4103/apc.apc_57_25","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite improvement in the outcome of the Norwood procedure, the prognosis of hypoplastic left heart syndrome (HLHS) remains problematic. The aim of this study was to assess the impact of pre- and perioperative factors and catheterization data on outcomes after the Norwood procedure.</p><p><strong>Subjects and methods: </strong>This case-control study included all patients who underwent the Norwood procedure for HLHS at Fukuoka Children's Hospital between January 2000 and October 2011. Subjects (<i>n</i> = 66) were divided into two outcome groups: survivors (<i>n</i> = 41) and nonsurvivors (<i>n</i> = 25). First, we compared the pre- and perioperative data. Second, we compared the catheterization data after the Norwood procedure.</p><p><strong>Results: </strong>The mean follow-up period was 40 months (range: 1.4-141). Overall, there was a 38% mortality, including early death. The pre- and perioperative data, as well as PaO<sub>2</sub> in room air at catheterization, were not significantly different. However, univariate analysis revealed that the incidence of home oxygen therapy to maintain oxygen saturation >80% was significantly higher in the survivors (<i>P</i> < 0.001). The right ventricular ejection fraction was higher in the survivors (48.7% ± 1.9%, mean ± standard error) than in the nonsurvivors (41.4% ± 2.8%, <i>P </i>= 0.041). The severity of tricuspid regurgitation (TR) and the pulmonary blood flow/systemic blood flow ratio were lower in the survivors than in the nonsurvivors. Multivariate logistic regression analysis identified severe TR as the only significant prognostic marker of mortality (<i>P</i> = 0.041).</p><p><strong>Conclusions: </strong>The severity of TR was associated with the prognosis of HLHS after the Norwood procedure.</p>","PeriodicalId":8026,"journal":{"name":"Annals of Pediatric Cardiology","volume":"18 2","pages":"100-104"},"PeriodicalIF":0.7000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12443387/pdf/","citationCount":"0","resultStr":"{\"title\":\"An 11-year single-center experience of Norwood procedures in the neonates with hypoplastic left heart syndrome and variants.\",\"authors\":\"Akihiro Nakamura, Yuichi Ishikawa\",\"doi\":\"10.4103/apc.apc_57_25\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Despite improvement in the outcome of the Norwood procedure, the prognosis of hypoplastic left heart syndrome (HLHS) remains problematic. The aim of this study was to assess the impact of pre- and perioperative factors and catheterization data on outcomes after the Norwood procedure.</p><p><strong>Subjects and methods: </strong>This case-control study included all patients who underwent the Norwood procedure for HLHS at Fukuoka Children's Hospital between January 2000 and October 2011. Subjects (<i>n</i> = 66) were divided into two outcome groups: survivors (<i>n</i> = 41) and nonsurvivors (<i>n</i> = 25). First, we compared the pre- and perioperative data. Second, we compared the catheterization data after the Norwood procedure.</p><p><strong>Results: </strong>The mean follow-up period was 40 months (range: 1.4-141). Overall, there was a 38% mortality, including early death. The pre- and perioperative data, as well as PaO<sub>2</sub> in room air at catheterization, were not significantly different. However, univariate analysis revealed that the incidence of home oxygen therapy to maintain oxygen saturation >80% was significantly higher in the survivors (<i>P</i> < 0.001). The right ventricular ejection fraction was higher in the survivors (48.7% ± 1.9%, mean ± standard error) than in the nonsurvivors (41.4% ± 2.8%, <i>P </i>= 0.041). The severity of tricuspid regurgitation (TR) and the pulmonary blood flow/systemic blood flow ratio were lower in the survivors than in the nonsurvivors. Multivariate logistic regression analysis identified severe TR as the only significant prognostic marker of mortality (<i>P</i> = 0.041).</p><p><strong>Conclusions: </strong>The severity of TR was associated with the prognosis of HLHS after the Norwood procedure.</p>\",\"PeriodicalId\":8026,\"journal\":{\"name\":\"Annals of Pediatric Cardiology\",\"volume\":\"18 2\",\"pages\":\"100-104\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12443387/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Pediatric Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/apc.apc_57_25\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Pediatric Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/apc.apc_57_25","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/29 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
An 11-year single-center experience of Norwood procedures in the neonates with hypoplastic left heart syndrome and variants.
Background: Despite improvement in the outcome of the Norwood procedure, the prognosis of hypoplastic left heart syndrome (HLHS) remains problematic. The aim of this study was to assess the impact of pre- and perioperative factors and catheterization data on outcomes after the Norwood procedure.
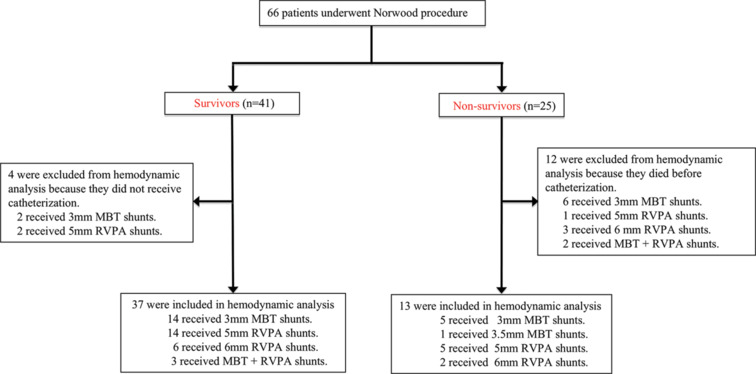
Subjects and methods: This case-control study included all patients who underwent the Norwood procedure for HLHS at Fukuoka Children's Hospital between January 2000 and October 2011. Subjects (n = 66) were divided into two outcome groups: survivors (n = 41) and nonsurvivors (n = 25). First, we compared the pre- and perioperative data. Second, we compared the catheterization data after the Norwood procedure.
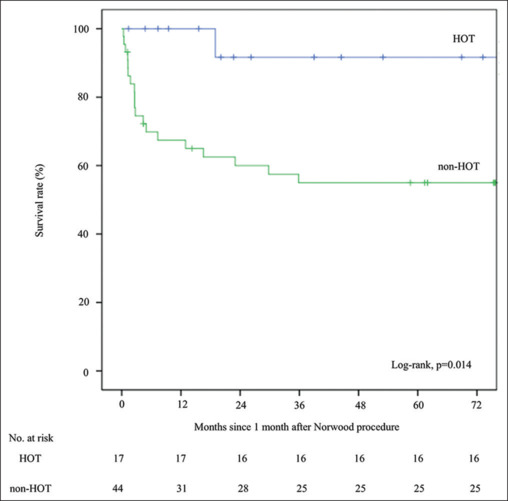
Results: The mean follow-up period was 40 months (range: 1.4-141). Overall, there was a 38% mortality, including early death. The pre- and perioperative data, as well as PaO2 in room air at catheterization, were not significantly different. However, univariate analysis revealed that the incidence of home oxygen therapy to maintain oxygen saturation >80% was significantly higher in the survivors (P < 0.001). The right ventricular ejection fraction was higher in the survivors (48.7% ± 1.9%, mean ± standard error) than in the nonsurvivors (41.4% ± 2.8%, P = 0.041). The severity of tricuspid regurgitation (TR) and the pulmonary blood flow/systemic blood flow ratio were lower in the survivors than in the nonsurvivors. Multivariate logistic regression analysis identified severe TR as the only significant prognostic marker of mortality (P = 0.041).
Conclusions: The severity of TR was associated with the prognosis of HLHS after the Norwood procedure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


